Administering insulin
There are four primary methods for administering insulin: Injections, insulin pumps, artificial pancreas systems/automated insulin delivery systems, or inhaler.
Injections
Many people manage type 1 diabetes (T1D) with multiple daily injections (MDI).
Syringes and pens are used for multiple daily injection (MDI) therapy. This typically involves a combination of both basal (long-acting) and bolus (rapid-acting) insulins. Injections are administered to the thigh, buttocks, abdomen, or upper arms.
In addition to traditional syringes, smart insulin pens are an option. Smart insulin pens and pen caps are devices used to track insulin doses for people who use MDI.

Insulin pumps
Insulin pumps are small devices that deliver a continuous supply of insulin through a tiny tube (cannula) inserted under the skin, typically in the upper thigh, abdomen, lower back, or tricep. The pump itself is worn outside the body and is programmed to deliver basal (long-acting) insulin continuously, mimicking the background insulin secretion of a healthy pancreas. Additionally, it allows the user to deliver bolus (short-acting) doses of insulin during meals and to correct high blood sugars.
Today, most pumps have the option to become artificial pancreas or automated insulin delivery systems, which automatically adjust insulin delivery based on real-time glucose readings.

Automated insulin delivery systems
Thanks to decades of work by Breakthrough T1D, people with T1D are now able to use artificial pancreas or automated insulin delivery systems to manage their T1D. These systems combine the technology of a pump with that of a continuous glucose monitor (CGM) to adjust insulin delivery based on real-time glucose readings, giving less insulin when blood sugar is low and more insulin when blood sugar is high.
Clinical research has demonstrated conclusively that individuals on these systems are able to more effectively manage their blood-glucose levels than those on multiple daily injections or standard insulin pump therapy.

Inhaled insulin
Afrezza, a quick-acting inhaled insulin, can be an alternative to injectable pre-meal insulin. It is inhaled immediately before a meal. It is FDA-approved for people 18 and over who have type 1 or type 2 diabetes. There are other criteria for use that your physician and diabetes care team can provide.
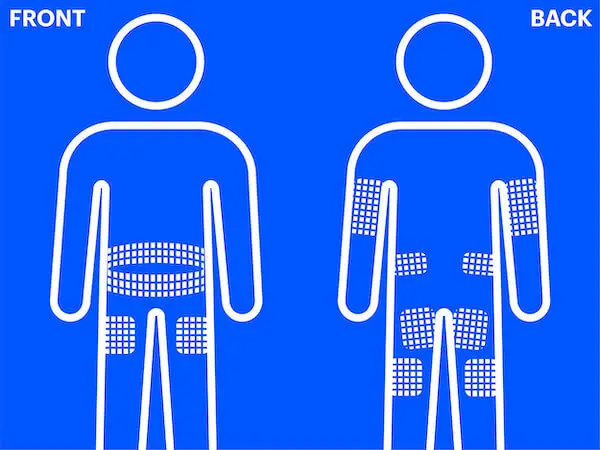
Rotating injection sites
It is important to rotate the location on your body where you inject insulin or place your insulin pump infusion site. If you don’t rotate the sites, the fatty tissue under your skin can be affected.
If insulin is injected or infused into the same part of the skin repeatedly, the skin becomes lumpy. This is called lipohypertrophy. If insulin is injected into the lumpy area, it won’t be absorbed consistently.
To avoid lumpy skin, make sure you pick a different area of skin for each injection or pump infusion site. Ideally, you should aim to keep each new site at least two inches away from your previous sites.
Types of insulin
Basal insulin
Basal, or long-acting, insulin provides a low level of insulin in the blood at all times. It starts working about an hour after injection and tends to lower glucose levels for 24 to 40 hours.
Bolus insulin
Bolus, or rapid-acting, insulin is administered at mealtimes and to manage high glucose levels. Rapid-acting insulin starts working about 15 minutes after administration, peaks (or is at maximum effectiveness) in about 60 to 90 minutes, and continues to work for 3 to 5 hours after administration.
Get support
Find your local chapter, attend an event, or join an online community summit to connect with other people living with type 1 diabetes.