Living a full and healthy life with type 1 diabetes (T1D) became clear to Matt Edgington when he was a teenager. He had been living with T1D since the age of 4, but his teenage years brought frustration and burnout. He didn’t check his blood sugar enough or administer the right amounts of insulin, resulting in a less-than-ideal A1C. “Coupling hormones with an attitude-filled teenager was just a recipe for disaster,” he said. “I wish I could say that was some kind of wake-up call, but it really wasn’t.”
Around that time, Matt started riding mountain bikes with his older brother and friends. That was the start of a major shift in his life. “As I started to ride more, everything just started to click: the better my blood sugar was, the better I was able to ride. The more I rode, the easier it was to control my blood sugar. It became a revolving door that had a huge impact on my life.”
Team Mattman
Matt at his first Walk in 2000
When Matt was diagnosed with type 1 diabetes, it didn’t entirely come as a surprise. His father, Ruedy, was diagnosed with T1D in 1970 at age 12 (and told by his doctor that he wouldn’t live to be 18!). “It was obviously horrible for them, but it wasn’t like this brand new, unknown thing,” Matt said. “My dad had been managing his T1D for 30 years at that point, and my mom was familiar with the day-to-day life of it.”
The Edgingtons immediately got involved with Breakthrough T1D (then JDRF), starting a Walk team, Team Mattman, in their Reno, NV, chapter that continued for the next 14 years. “That was, hands down, my favorite day of the year, every year,” Matt said. “I used to autograph everyone on my team’s shirt!”
Grabbing fundraising by the handlebars
Three generations of the Edgington family at the 2019 Amelia Island Ride
As Matt got older, the Edgington family started looking for new ways to support the T1D community. “We still had a desire to be involved and continue to raise money, so, as a cycling family, our efforts naturally rolled over right into doing Rides,” Matt said.
Breakthrough T1D Ride also felt like something he could stamp as his own way to raise money and awareness for type 1 diabetes after his family had led efforts for so many years. “Riding at the front with the fast riders, and now being a Ride coach, feels like the first contribution that I am making on my own to the organization,” he said.
Ride coaching was a natural evolution for Matt, who now lives in Utah. “It’s the most outdoorsy community I have ever been around, so it felt like a huge opportunity to grow the Ride program here,” he said.
To date, Matt’s parents have done more than 25 Rides. This year will mark Matt’s 15th Ride.
Confidence through cycling
Cycling has given Matt confidence he never imagined. He recently completed a 100-mile mountain bike race in Leadville, CO, and considers that his biggest T1D success. “Training and completing that ride was a huge statement that a person living with type 1 diabetes can do anything.”
But to Matt, now more than 25 years into his T1D journey, there is still no cycling event quite like the Breakthrough T1D Ride. “It’s an inspiration: the people with T1D all on their bikes fighting for the same cause.”
Your story matters
Living with T1D looks different for everyone. We want to hear your story: the highs, the lows, the challenges you’ve overcome, and the people who have supported you on your journey.
When your body doesn’t have enough insulin to use the sugar in your blood, it breaks down fat for energy. This produces chemicals called ketones, which make your blood more acidic. Elevated ketone levels often occur when blood sugar readings are high. Very high levels could lead to diabetic ketoacidosis, or DKA, a dangerous condition that demands immediate medical attention.
Ketones and diabetic ketoacidosis (DKA)
Diabetic ketoacidosis is a serious condition in which an insulin-deprived body seeks energy from stored fat. When ketones build up, the result is acidosis (too much acid in the blood). If not treated, this can lead to death. A person in DKA usually has elevated blood glucose levels (>240 mg/dL), but not always.
Signs of diabetic ketoacidosis include:
Vomiting
Stomach or abdominal pain
Difficulty breathing
Confusion
Extreme sleepiness
Sweet-smelling or fruity breath
When to check for ketones
Many doctors advise checking for ketones if you are ill, especially if you are vomiting, have stomach pain, or have a fever. It’s also important to monitor ketones when blood glucose is above target—for example, higher than 240 mg/dL for three hours if you use an insulin pump or an automated insulin delivery (AID) system, or higher than 300 mg/dL for three hours if you do multiple daily injections (MDI).
If your blood sugar is above 240 mg/dL, you should test for ketones before exercising. The presence of ketones in someone with T1D shows that there’s not enough insulin in the body to use the sugar. In general, it’s okay to exercise with trace or small ketones, but if ketone levels are moderate or large, exercise should be delayed until ketone levels are lower. Contact your diabetes care team for advice about activity and exercise when ketones are detected.
How to check for ketones
You can check for ketones in urine or in blood. Monitoring blood ketones is preferred over urine ketones because it provides more precise information about your ketone levels. Blood ketone strips can be expensive, so urine ketone test strips are adequate. Keep in mind that because urine may have been in the bladder for some time, the results from urine tests may show levels that are either higher or lower than the ketone levels currently circulating in your body.
It is also very important to know that urine test strips degrade over time. If you are using urine ketone strips, look at expiration dates carefully and discard containers open longer than 6 months.
What ketone levels mean
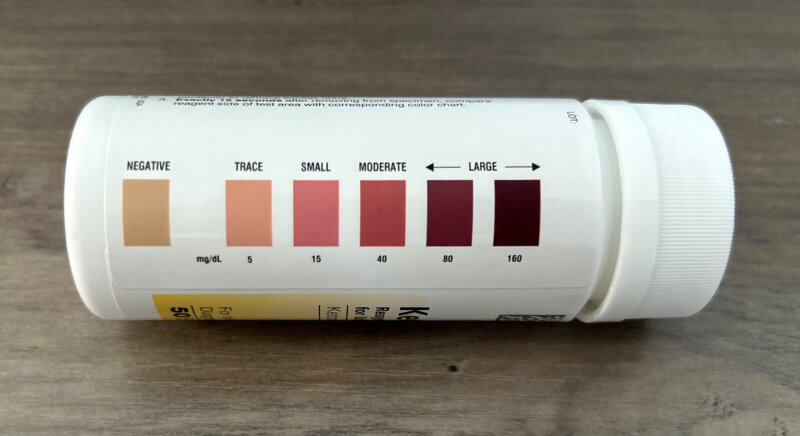
Ketone levels can indicate if you are at risk of diabetic ketoacidosis. At-home urine test strips will change color to show the level of ketones in urine. They typically report results as negative, trace, small, moderate, or large.
Urine ketone level
Indication
Negative or trace
Considered normal for people with type 1 diabetes.
Small
Closely monitor your ketones. If you are experiencing illness, call your diabetes care team and follow the plan you have in place for treating ketones.
Moderate
Indicates risk of diabetic ketoacidosis. Call your diabetes care team right away and follow the plan you have in place for treating ketones.
Large
Considered a medical emergency. Call your diabetes care team immediately and possibly go to the emergency room.
Blood ketone meters provide a number to indicate ketone levels. The following ranges are generally used:
Blood ketone level
Indication
Less than 0.6mmol/L
Considered normal for people with type 1 diabetes.
0.6 to 1.5 mmol/L
Closely monitor your ketones. If you are experiencing illness, call your diabetes care team and follow the plan you have in place for treating ketones.
1.5 to 3.0 mmol/L
Indicates risk of diabetic ketoacidosis. Call your diabetes care team right away and follow the plan you have in place for treating ketones.
More than 3.0 mmol/L
Considered a medical emergency. Call your diabetes care team immediately and possibly go to the emergency room.
Treating elevated ketones
If testing shows you have elevated ketones in urine or blood, follow the plan you and your diabetes care team have in place for treating ketones. Treatment typically includes increasing insulin and fluid intake.
Ketones and illness
Being sick is never fun, but for people with T1D it can pose extra problems and put you at increased risk of DKA.
When a person gets sick, their body is under stress. During times of mental or physical stress, like when sick with the flu or a serious infection, the body makes and releases stress hormones to fight illness. This can affect your blood sugar. On these days, you will need to monitor your blood sugar and ketone levels very closely, usually every 2-4 hours.
Breakthroughs in DKA prevention and ketone monitoring
Breakthrough T1D is spearheading research into new technologies to reduce the risk of diabetic ketoacidosis as much as possible for people with T1D.
Screening is essential to detect T1D early and prevent DKA at diagnosis. It can be particularly dangerous if a person isn’t aware that they should monitor their blood glucose or ketones. Recently published consensus guidelines—authored by Breakthrough T1D staff and other international experts—provide information to healthcare providers (HCPs) about monitoring people who test positive for T1D autoantibodies but are pre-symptomatic. This will help HCPs make the best care decisions possible for screening individuals and reducing the risk of DKA.
Breakthrough T1D’s Improving Lives program focuses on developing easier and more accurate ways to measure ketone levels. Advancements have been made in continuous ketone monitoring (CKM), which, similar to continuous glucose monitoring (CGM), could allow for constant, real-time ketone measurements. These devices have the potential to significantly reduce the risk of DKA by informing people when ketone levels are rising so they can act before an emergency occurs. Integration with CGMs would allow for even greater blood glucose and ketone control.
When living with type 1 diabetes, be sure to consistently check your ketone levels to prevent DKA. Keep an eye out for the latest breakthroughs in devices and technology that will soon make this easier than ever!
In 1968, Dennis Goldensohn was a 16-year-old working at White Castle in Queens, NY. He started experiencing extreme thirst and tried quenching it with cola from the soda fountain. After a few weeks of on-and-off symptoms, he went to his family doctor. “He was the old Marcus Welby type of guy, with the rolled-up sleeves of a white Oxford shirt, wearing a tie and a stethoscope around his neck,” Dennis recalled. “And he told me to see an endocrinologist as soon as possible.”
At the endocrinologist, Dennis’ blood sugar was tested via urine test strips—the number was off the charts. The doctor said to his parents, “Your son has juvenile diabetes and will be on insulin shots for the rest of his life.” He gave Dennis a vial of pork insulin and some 24-gauge syringes, showed him how to inject it, and sent him home with a pat on the back.
The next day, when Dennis had to administer his first injection, he had a moment of resolve. “I said to myself, ‘This is not going to get in my way. This is not something that is going to be a roadblock’.”
That day began Dennis’s 57-year journey of living a full and healthy life with type 1 diabetes.
Applying lived experience to type 1 diabetes
Dennis worked in the manufacturing industry for over 40 years and has used that experience to better manage his type 1 diabetes.
“In manufacturing, I did statistical process control,” he said. “With T1D, it’s not control, it’s management. You manage diabetes, so the bandwidth of your time in range is narrow.”
He also takes a practical approach to what lies ahead. While he praises technology like CGMs and automated insulin delivery systems, those are not the end game for him.
“In lean manufacturing, the present is what we call the ‘current state.’ We don’t like the current state; we want the ideal state, which would be cures.”
Reducing T1D stigma in the workplace
Dennis is very passionate about reducing the stigma of type 1 diabetes in the workplace. He recalls times when he would need to inject insulin at professional meetings. “People would ask me, ‘What are you doing?’ and I would reply, ‘I’m diabetic, and this is what I do.’” His matter-of-fact approach encouraged others in the workplace to advocate for themselves.
In the 1980s, Dennis held “Lunch and Learn” sessions at his workplace to support his co-workers living with T1D. “My experience of one benefited 20 others,” he said. “If you’re a champion and a change agent, that makes all the difference.”
Giving back to the type 1 diabetes community
Since the 1970s, Dennis has been an avid advocate for our organization and the T1D community and has graciously volunteered as a photographer for his local Breakthrough T1D Walks, Community Summits, golf tournaments, and Galas.
He also deeply enjoys mentoring other people living with T1D, from the ages of 4 to 84. “I want to show them that everything can work out,” he said. “Everything is possible.”
Dennis encourages his fellow “type 1 diabetes veterans” to share their experiences and support with the T1D community. “It will benefit you and everyone else facing the condition. You have to give of yourself for yourself.”
Tips from a T1D veteran
Dennis is proud of his healthy life with type 1 diabetes and says there are a few important things that have helped him along the way:
A positive attitude “A positive mind leads to positive health outcomes.”
A deep understanding of T1D “The more knowledge you have, the easier it is to manage because you have more answers.”
A supportive community “Whether it’s your spouse, your sibling, or even your neighbor, a strong ‘nucleus’ is important for a healthy life.”
Dennis’s optimism continues to shine through in everything he does.
“At heart, I’m still a kid from Brooklyn,” he said. “I still feel like I’m 16 years old and can play stickball and sing doo-wop harmony on the street corner. I’m going to be here forever—that’s my attitude. Type 1 diabetes is still not getting in my way!”
Your story matters
Living with T1D looks different for everyone. We want to hear your story: the highs, the lows, the challenges you’ve overcome, and the people who have supported you on your journey.
We may never lose the memory of sitting in a hospital room when the doctor told us that our 15-month-old son Matthew, a baby with his entire life in front of him full of open possibilities, had type 1 diabetes (T1D). We were told he would spend the rest of his life monitoring his blood sugar, receiving insulin, and being very aware of things that many of us never have to think about, like his glucose level and beta cells in his pancreas.
When we were connected with Breakthrough T1D, it was an awakening. We met people going through the same roller coaster of emotions that we were. We met people who told us, “We understand,” in a way that our family and friends could not.
The road also travels both ways. We have been fortunate enough to speak to the parents of newly diagnosed children and look into their eyes. We have been able to provide a comforting word or hug to someone who felt the same way we did after diagnosis.
Within one month of Matthew’s diagnosis, we signed up for the Breakthrough T1D Walk. Instead of feeling helpless because there is no cure, we looked at it as discovering a new cause that we had to fight for. It was something that was within our control to help make his life better.
So why do we walk with Breakthrough T1D? Because of a memory.
A memory of Matthew standing on stage at the Breakthrough T1D Walk, watching him take the microphone to start the event countdown.
But most of all, we walk because of the memory of Matthew saying, “I wish I did not have diabetes,” and knowing that the research funded by Breakthrough T1D will improve his way of life and take us a step closer to his wish of finding cures.
Walk toward cures
Breakthrough T1D Walk is the largest global event for the T1D community, driving research, advocacy, and support to improve lives while funding cures research.
Outside the Cammett family’s Michigan home sat a new toy truck. John, around six years old, admired its sturdy metal frame, fresh rubber wheels, and bright yellow decals. But it would not stay that way for long.
John and his two brothers were athletic, boisterous, and yes, at times, destructive. After the truck was thoroughly battered, John’s mother, Barbara, began her work on the piece. She was creative and artistic and knew just what to do. With paint brushes in hand, she covered the damaged truck in a collage of color and something new emerged. It was no longer a wreck, it was a work of art.
John Cammett, now 62, says he’ll always remember that day and the special lesson that came from it.
“Even with all that destruction, she could make something look beautiful,” he said.
Like mother, like son
John’s mom was diagnosed with type 1 diabetes (T1D) in her 30s and passed away in 2021 at age 89. She inspired John, who also lives with T1D, to become a champion for others with the condition. John has since become a longtime volunteer, leader, and advocate for Breakthrough T1D—providing transformational support of our mission.
In recognition of his deep commitment, the Breakthrough T1D Center of Excellence in New England was recently named for his mother. The center will now be known as the Breakthrough T1D Barbara Dewey Cammett Center of Excellence in New England. John helped establish the center and provided foundational support for Project ACT (Accelerate Cell Therapies), Breakthrough T1D’s initiative to make cell therapies as cures for T1D a reality.
My mom was the strongest person I’ve ever known—a real warrior. Even back then, with limited technology, she never let T1D set her back.”
John Cammett,Co-Chairman and Founding Partner of Realterm and Passionate Seed Funder of The Breakthrough T1D Barbara Dewey Cammett Center of Excellence in New England
Honoring her positive spirit
Since its inception, the Breakthrough T1D Barbara Dewey Cammett Center of Excellence in New England has made significant progress advancing islet cell-based T1D research, enhancing the understanding of the immune response following islet transplantation to prevent rejection, and creating genetically modified islet cells that could withstand the immune attack after transplantation into people living with T1D.
From left: Director of the Breakthrough T1D Barbara Dewey Cammett Center of Excellence in New England David M. Harlan, M.D.; John Cammett; and Breakthrough T1D CEO Aaron J. Kowalski, Ph.D, together at an event where the Center’s new name was shared.
The breakthrough research happening at the center—one of five Breakthrough T1D Centers of Excellence around the world powering advances to deliver cures and life-improving breakthroughs for T1D—is particularly inspiring to John. He takes pride in knowing that the center he helped establish will not only advance this important work but also honor his mother’s positive spirit and enduring legacy.
“You can’t be a researcher without optimism—every breakthrough stands on the back of countless failures. My mom lived the same way. She was the most optimistic person I’ve ever known, never said a bad word about anyone, and kept going no matter how hard things got. Just like the researchers pushing forward every day, she stayed focused, kind, and hopeful through it all.”
A beacon of strength
John remembers his mom as a woman whose generous heart, zest for life, and unwavering optimism inspired everyone she met.
She managed T1D for nearly 60 years with grace, determination, and a smile. Known for her vibrant personality, Barbara embraced life fully. You could often find her cheering on her Wisconsin Badgers, painting beautiful art, volunteering in her community, and effortlessly outdriving her husband on the golf course.
Barbara Dewey Cammett (seated center) with her three sons: John (standing center), Bryan (standing, left) and Stuart (seated, right).
Her kindness, resilience, and passion for connecting with others made her a beloved friend, devoted wife, and beacon of strength to those navigating life with T1D.
“I wish I could have done this while she was still with me,” John said. “But I know she’d look back and smile. She wanted to help everyone she could. That spirit lives on.”
By: Adam Baker
The summer season means a few extra things to consider when it comes to managing type 1 diabetes (T1D). Our guide is here to help!
5 tips for summer with type 1 diabetes
Stay hydrated. Hot weather can quickly dehydrate anyone. To avoid the blood-sugar spikes it causes, be sure to drink water throughout the day.
Test blood-sugar levels frequently. Since hot temperatures can cause unusual swings in blood-sugar levels, it’s a good idea to test your blood sugar more often than usual.
Protect your gear. Keep your pump covered and your insulin cool! Heat makes insulin less effective and can cause pumps to malfunction. There are cooling cases specifically for insulin that can help you manage your supply.
Pack snacks. Before any summer road trips or outings, stock up on low snacks. Snacks can help prevent blood-sugar lows. And try to stay on your food schedule, no matter what the trip throws at you.
Exercise in the mornings or nights. Plan your outdoor exercise for the cooler parts of the day. Exercising in the heat can cause heat exhaustion and make staying in a healthy range difficult. Even at these times, sweating is likely when working out. Because too much moisture can damage a pump, be sure to keep an eye on it.
Insulin and heat
Insulin is a protein; like any other protein, it breaks down in heat, making it ineffective.
The temperature at which your insulin is at risk of damage is 93°F.
That temperature might seem extreme, but after two hours in a hot car, playing sports outside, or even just lying out on a beach towel, your insulin supply could be in trouble. Be sure to keep it cool and change the insulin in your pump regularly.
Wear sunscreen
Everyone should protect their skin from harmful UV rays, but with T1D, wearing sunscreen is extra important. Why? Sunburns can cause extra, unneeded stress on the body that can cause blood-sugar spikes.
For the best sun protection, use SPF 30 or higher and reapply frequently when outside.
Summer heat’s impact on blood sugar
Unfortunately, heat can cause both unexpected highs and lows in blood-sugar levels.
Dehydration is common in the summer and can lead to spikes when blood glucose becomes more concentrated due to decreased blood flow through the kidneys.
The heat can also cause dips in blood-glucose levels. As the temperature rises, the body’s blood vessels expand, speeding up insulin absorption and increasing the risk of hypoglycemia. This is especially true while exercising, as working out increases blood flow.
Summer travel checklist
What’s in your summer travel bag? Whether you’re on a day trip to the beach or jet setting somewhere far away, here are some T1D essentials to add to your packing list:
A travel letter from your doctor with written approval to travel with insulin and syringes (recommended)
Insulin
Syringes
Insulin pens
Test strips
Lancets
Ketone test strips
Pack twice as much medication and supplies as you think you’ll need (just in case!)
Back-up snacks for quick carbs
Emergency glucagon
Equipment, including blood glucose meters, continuous glucose monitors (CGMs), and insulin pumps
If you use an insulin pump, many manufacturers offer loaners for travel. Ask for one as a back-up!
Keep all of the above, especially your insulin, in a carry-on bag. Medications should be kept in a clear plastic bag, ready for airport security. Don’t store insulin or a CGM in checked luggage—cargo holds can have extreme temperatures!Visit our Travel Guide for more helpful tips.
Cocktails and carbs: how to drink safely with T1D
T1D should not keep you from a good time and, perhaps, a nice glass of wine. Just like anyone partaking in alcohol, there are a few things to be aware of.
Be mindful of your alcohol consumption, especially in the sun, as it can affect your body’s ability to regulate its temperature. Because certain drinks can have unexpected impacts on blood sugar, you can always talk it through with your doctor. In general, stick to low-sugar options, stay hydrated (with water!), and don’t drink on an empty stomach.
When the temperature begins to rise and we start spending more time outdoors, that means cookout season is just around the corner. It’s also a great time to try some new type 1 diabetes-friendly recipes.
We asked you—members of the Breakthrough T1D community—for your favorite summer recipes and you delivered. Enjoy!
No-cook recipes
Type 1 diabetes-friendly recipes that are perfect for when it’s too hot to cook!
Ingredients for the salad:
1 cup dry green lentils
1 English cucumber, chopped
1 cup cherry tomatoes, halved
½ red onion, diced
½ cup fresh mint, chopped
1 can hearts of palm, chopped
Ingredients for the dressing:
1/3 cup olive oil
2 limes, juiced
2 cloves garlic, mashed
1 tablespoon Dijon mustard
1½ teaspoons sea salt
1 teaspoon ground black pepper
Directions:
Start by preparing your lentils; rinse and drain your lentils thoroughly, then add them to a saucepan with three cups of water and a generous pinch of sea salt. Bring the lentils to a boil, then once they’re boiling, cover the pan, reduce the heat to “low”, and let your lentils simmer for about 25 minutes. While your lentils are simmering, prepare the rest of your salad. Wash and chop your cucumber, tomatoes, red onion, hearts of palm, and mint, and set them aside. Then, in a separate bowl, add all of your dressing ingredients together and whisk them to combine. Taste and adjust salt and pepper levels as needed / desired.
Once your lentils are finished, strain the water from them and rinse them with cold water to cool. Then, add your cooled lentils to a large bowl along with the rest of your vegetables. Finally, pour your dressing on top and toss to fully combine. Once your salad is done, serve it right away, or store any leftovers in an airtight container, in the fridge, for up to one week. Enjoy!
Estimated carb count per serving: ~10g
Contributed by Jill Waller
Ingredients:
1 red onion, chopped
1 pint cherry tomatoes, sliced in halves
1 avocado, pitted and cut into 1/4 inch pieces
1 can of black beans, drained and rinsed
1 can of fresh cut, whole kernel corn, drained
Oil and balsamic vinegar to taste
Ground black pepper to taste
1 pinch of salt
Directions:
Combine/mix all ingredients in a bowl. Serves six as a side dish. Double all ingredients to serve 12. Keeps well refrigerated for a day, travels well. Enjoy!
Estimated carb count per serving: ~15g
Contributed by Francesca Lito
Ingredients:
6 cups chopped fresh broccoli
1 package bacon, cooked and crumbled
1 cup golden raisins
½ chopped onion
1 cup sunflower seeds
1 cup mayonnaise
¼ cup sugar substitute (erythritol or Stevia)
2 tablespoons white wine vinegar (or plain white vinegar)
Directions:
In a medium mixing bowl, whisk together mayonnaise, sugar substitute, and vinegar to make the dressing. In a large mixing bowl, combine broccoli, cooked bacon, chopped onion, raisins, and sunflower seeds. Pour dressing over the broccoli mixture, toss/stir to coat dry ingredients with dressing. Refrigerate until ready to serve.
Pro Tip: This salad tastes better after the flavors have time to meld for a few hours.
Estimated carb count per serving: ~18g
Contributed by Pat Goldstein
Ingredients:*
Cucumbers
Cider vinegar or vinegar of your choice (ex: red wine, etc.)
Vegetable or olive oil (optional)
Water
Salt & pepper to taste
Other seasonings/add ins (optional). Suggest dill and or thinly-sliced scallions or fine-chopped red onions.
*No measurements. This is a “taste-and-adjust-to-your-liking” kind of recipe.
Directions:
Slice cucumbers the way you like them. Pare cucumbers (or not, based on your preference). The other ingredients are going to cover and flavor the cucumber. Start with the vinegar. Add a tablespoon or two of oil. Oil can be left out completely if you prefer. Add enough water to adjust the acidity from the vinegar to your liking. Season optionally. A pinch of salt and a grind or two of pepper. Then whatever else you’ve chosen to taste. If you sample and like it, you’re good. It is ok if the vinegar doesn’t taste overly strong. Mix cucumbers and dressing in bowl. Toss to evenly coat cucumbers. As the cucumbers sit they will absorb the flavor. But do make sure it’s vinegary enough to give cucumbers some good zing!
Pro tip: If you mix dressing in a measuring cup, you can stir and sample to see what else you might need
Estimated carb count per serving: ~2g
Contributed by Ellen Warsaw
Ingredients:
1 bunch of medium-sized, seedless green grapes
1 package of sugar-free flavored gelatin mix (choose your favorite flavor)
Directions:
Thoroughly wash the grapes. Pluck from stems, but do not dry. Place wet grapes into freezer bag. Pour gelatin mix over the wet grapes in the bag. Seal bag. Shake well to coat grapes with gelatin mix. Freeze for four hours.
Estimated carb count per grape: ~1g
Contributed by Wendy Rose
Ingredients:
3/4 cup of full fat plain Greek yogurt
½ cup (or 100 grams) frozen strawberries
1 scoop vanilla whey protein
1-3 tablespoons of water
Ice cubes (optional)
Directions:
Add all ingredients to blender. Blend. Add water based on desired thickness. If too thin, add a few ice cubes.
Melt almond butter and organic honey/agave in microwave for 40 seconds and then stir.
Add in Arbonne protein powder, brown Rice Krispies, and oats. Mix up with hands. Roll into approximately 20 small balls. Place balls on wax-paper or parchment paper-lined tray and place in fridge for at least an hour. After balls have chilled, remove from tray and place in big bowl. Refrigerate. Enjoy.
Estimated carb count per serving: ~25g
Contributed by Bek Hoskins
Summer Barbecue Guide
Our Summer Barbecue Guide offers tips and carb counts so that you and your loved ones can make the most of every moment.
Type 1 diabetes-friendly recipes for when you don’t mind cooking a bit!
Ingredients:
1lb asparagus
1lb thick cut bacon
Your seasoning of choice
Directions:
Wrap one slice of bacon around three Asparagus stalks. Season with your choice of seasoning. Cook on grill until asparagus is tender or cook in oven on a pan at 350 degrees for about 20 minutes.
Spray waffle iron with high-heat, non-stick cooking spray. Heat waffle iron. Mix mozzarella cheese, eggs, and baking powder until blended. Pour mixture into waffle iron. Bake on one cycle or for 5 minutes. Remove from iron. Add toppings.
Estimated carb count per serving: ~3g (without toppings)
Contributed by Julia Orlicky
Ingredients:
1lb (one box) of bowtie pasta (or other shape)
3 stalks of celery chopped
1/2 yellow onion finely diced
1 cucumber, seeded, chopped
1 cup light mayo
2 tsp white vinegar
1 tsp sugar
1 tsp celery seed
1/4 tsp ground mustard
1/4 tsp salt
1/4 tsp ground black pepper
Directions:
Cook pasta until al dente; drain. Whisk mayo, vinegar, and seasonings together in a bowl. Combine cooked pasta with chopped vegetables. Add dressing and mix until pasta and veggies evenly coated with dressing. Cover bowl and refrigerate to let flavors develop. Toss/stir again before serving.
Estimated carb count per serving: ~40g
Contributed by Amanda Gottleib
Ingredients:
2 medium zucchini, sliced 1/4″ thick
2 medium yellow squash, sliced 1/4″ thick
2 medium eggplant, sliced 1/4″ thick
2-3 tablespoons olive oil
1-2 large tomatoes sliced 1/4″ thick
1 cup cherry tomatoes, halved
2 balls fresh mozzarella cheese (or more, if you’d like!)
2 tablespoons aged balsamic vinegar
4-5 leaves fresh basil, chopped
Salt and pepper, to taste
Directions:
Heat the grill to a medium heat.
Brush the zucchini, squash, and eggplant with the olive oil and sprinkle lightly with salt and pepper. Grill for 4-5 minutes on the first side before flipping them and grilling for an additional 2-3 minutes on the other side until slightly softened. Transfer the grilled vegetables to a sheet pan to rest.
Slice the mozzarella into 1/4″ slices. Use a large plate or platter to layer the grilled veggies, tomatoes, and mozarella. Sprinkle chopped basil on top. Drizzle with balsamic vinegar and olive oil. Sprinkle with additional salt and pepper, if desired. Serve at room temperature or slightly chilled.
Estimated carb count per serving: ~10g
Ingredients:
¼ cup brown sugar or coconut sugar
2 tablespoons butter
2 teaspoons vanilla
1 egg
2 cups almond flour
½ tablespoon baking soda
¼ tablespoon salt
⅓ cup chocolate chips
Directions:
Preheat oven to 350°F.
Mix ingredients in a large bowl. Make ~24 small cookies on a non-stick cookie sheet.
Bake for 10-12 minutes until golden brown. Let cool and serve.
Estimated carb count per serving: ~4g
Contributed by JoAnn Kjep
Have a recipe you’d like to share? Email us your type 1 diabetes-friendly recipes at Social@BreakthroughT1D.org.
People with type 1 diabetes (T1D) are at an increased risk of developing other autoimmune diseases, with celiac disease being the most common. In fact, approximately 6% of those with T1D also have celiac disease. Here, we explore what celiac disease is, how to treat it, and its connection to T1D.
What is celiac disease?
Celiac disease is an autoimmune condition in which a person’s body cannot digest foods that contain gluten, a protein found in wheat, rye, barley, and some oats. If a person with celiac disease consumes gluten, their immune system reacts by attacking the lining of the small intestine (part of the gastrointestinal tract).
Because most essential nutrients in food are absorbed in the small intestine, the damage caused by celiac disease can lead to decreased nutrient absorption, resulting in nutritional deficiencies. Over time, these deficiencies can cause secondary issues, including slow growth, anemia, and osteoporosis.
What are the symptoms of celiac disease?
Gastrointestinal symptoms of celiac disease include:
gas and bloating
diarrhea
vomiting
stomach pain
weight loss
dermatitis herpetiformis (skin rash)
A survey conducted by Beyond Celiac found that neurological and physiological symptoms of celiac disease are often just as common as GI symptoms. The most commonly reported non-GI symptoms include brain fog, headache, joint pain, and fatigue.
How is celiac disease diagnosed?
Celiac disease diagnosis requires a medical evaluation of symptoms. This may require a blood test to measure levels of specific autoantibodies and a tissue biopsy from the small intestine to check for damage to the lining, often performed via endoscopy.
What is the connection between celiac disease and type 1 diabetes?
Celiac disease and type 1 diabetes share a common genetic background linked to the human leukocyte antigen (HLA) genotype. Approximately 95% of individuals with type 1 diabetes and nearly 99% of those with celiac disease carry the HLA class II genes DQ2 and DQ8. However, most people with these high-risk genes do not develop T1D or celiac disease.
“The reasons why some people with type 1 diabetes develop celiac disease while others do not, despite the common genetic background, is an area of active research,” says Farid Mahmud, MD, from the Hospital for Sick Children in Toronto. “The T1D population is also unique when it comes to celiac disease because they are largely asymptomatic.”
Because of this close genetic relationship, screening for celiac disease is frequently recommended in people living with T1D, regardless of age. “There is often an incorrect perception of celiac disease with type 1 diabetes as a largely pediatric condition,” Mahmud said. “In reality, autoimmune comorbidities increase with age, and data from our large screening study showed that adults with type 1 diabetes had higher celiac disease-seropositivity rates than children.”
Screening for celiac disease in those with type 1 diabetes is crucial because, according to a recent study, only 10% of people with celiac disease develop “classic” severe digestive symptoms; most have mild symptoms, vague neurological or physiological symptoms, or may even be asymptomatic.
Autoimmunity Screening for Kids (ASK) Program
T1D and celiac disease are the two most common autoimmune diseases of childhood. Breakthrough T1D supports the Autoimmunity Screening for Kids (ASK) Program, based at the Barbara Davis Center for Diabetes in Denver, CO. The program offers free screening to all U.S. children and adults to detect T1D or celiac disease.
The goals of ASK are:
Find early signs of type 1 diabetes or celiac disease in children before they get very sick
Offer close monitoring, education, and early treatment when needed
Offer participation in studies of new interventions that might stop or slow the progression of the disease
Increase public awareness of T1D and celiac disease
While there is no cure for celiac disease, it can be effectively managed through a strict gluten-free diet. Removing gluten (wheat, rye, barley, and some oats) from the diet allows the small intestine to heal, improving nutrient absorption.
Many foods are naturally gluten-free, including:
Fruits
Vegetables
Beef
Poultry
Fish
Nuts
Eggs
Today, gluten-free bread, pasta, and even pizza crust are widely available in most grocery stores. Restaurants have also become more accommodating to gluten-free diets. FindMeGlutenFree.com is a good resource for finding restaurants in your area with gluten-free options.
Going gluten free with type 1 diabetes
Individuals with T1D who are diagnosed with celiac disease may notice a change in their blood-glucose control after starting a gluten-free diet. As gluten is removed, the gut lining can heal, leading to improved absorption of nutrients, including carbohydrates. Pay special attention to blood-glucose levels until the body becomes more efficient at absorbing nutrients.
Gluten-free products tend to be higher in saturated fat, lower in protein and fiber, and have a high glycemic index, which could contribute to difficulties controlling blood sugar. Some individuals with type 1 diabetes may also require more insulin after being diagnosed with celiac disease. It is important to keep your T1D healthcare team informed about how you are managing your gluten-free diet and its effect on your blood-glucose levels.
Breakthrough T1D’s Improving Lives Program aims to ensure that people with type 1 diabetes (T1D) have the best quality of life possible until we realize cures. Daily T1D management is burdensome and demanding, and it can take a toll on mental and emotional health. That’s why providing psychosocial support to the T1D community is a key component to our Improving Lives work.
Experts convene at Breakthrough T1D’s Psychosocial Roundtable
To better understand the mental health needs of the T1D community, Breakthrough T1D and our partner, The Leona M. and Harry B. Helmsley Charitable Trust, co-hosted a Psychosocial Roundtable earlier this year, convening mental and behavioral health experts across the T1D care spectrum.
The goal was to understand how Breakthrough T1D can improve its efforts in the psychosocial space to provide the best possible resources so more people with T1D do better. Read on to learn about the current state of mental health care for the T1D community, what Breakthrough T1D is doing to help support the mental and emotional wellbeing of people with T1D, and the challenges we still face.
Mental wellbeing challenges for people with T1D
Diabetes distress, depression, anxiety, and disordered eating are the primary psychosocial conditions that people with T1D may experience. They can arise from the stress of day-to-day T1D management (such as insulin dosing and fear of hypoglycemia), a new T1D diagnosis, or long-term complications.
According to the American Diabetes Association, one in four people with T1D will likely experience high levels of diabetes distress, which itself can lead to worse blood sugar control. It is often associated with anxiety and, if left untreated, can develop into major depression. Diabetes distress more often impacts adolescents and young adults with T1D.
People with T1D may also develop eating disorders, often manifesting as anorexia, bulimia, or purposeful misuse of insulin to lose weight (diabulimia). These issues are more likely to occur in women or girls.
Addressing mental and emotional health needs for the T1D community
In recent years, there has been a surge in research addressing diabetes distress. In addition, Breakthrough T1D spearheaded an effort to support the publication of clinical guidelines for autoantibody-positive stage 1 or 2 T1D, which has an entire section dedicated to guidance for healthcare professionals (HCPs), families, and caregivers to provide psychosocial support.
Psychosocial interventions are structured programs led by trained professionals that can help alleviate mental and emotional distress. For example, a Breakthrough T1D-funded study is examining the use of cognitive behavioral therapy to address anxiety in presymptomatic T1D. This type of intervention may help ease fears caused by impending onset of T1D symptoms—and may even be applicable to people who might be too nervous to get screened.
The most successful models for mental health care in practice have been group-based, fully virtual, limited in time, and focused on emotions. To further elevate mental health interventions for the T1D population, Breakthrough T1D has developed a multi-pronged strategy to ensure that people with T1D can get the support they need:
Increase the number of trained psychosocial professionals.
Increase the number of available psychosocial interventions.
Improve implementation of psychosocial interventions into clinical practice.
Despite the availability and success of interventions that help manage mental health and T1D, there are still gaps in care that we need to work hard to overcome.
Existing challenges in mental health care for people with T1D
One of the most pressing barriers to incorporating psychosocial interventions into clinical practice is a lack of HCPs who are trained to provide mental health care to people with T1D. Many clinical settings don’t have the resources to support an additional behavioral health expert specifically for T1D, so T1D training programs must include an understanding of how to provide mental health support as part of comprehensive care.
Along these lines, many HCPs and families may not know that mental health support programs exist for people with T1D. Or, if they do, there may be logistical challenges for participants, such as time constraints or meeting location.
The T1D research community needs more scientific, data-driven research for psychosocial interventions. For example, there has been little research to date on disordered eating and T1D. An inquiry spearheaded by Breakthrough T1D affiliates in the U.K. determined that there is a significant gap in education, clinical guidelines, and recognized criteria for T1D-associated eating disorder diagnoses. Similarly, because diabetes distress is not considered a mental health disorder, there are no clinical criteria associated with it—making diagnosis and treatment even more difficult.
Because of these challenges, the rates of screening and use of evidence-based mental health support programs for people with T1D varies significantly between clinics. Even more, there is the persistent issue of mental health care reimbursement—if it’s not covered by insurance, people with T1D may choose to not utilize the programs available to them.
How Breakthrough T1D is filling these gaps
Thanks to the experts who convened at the Psychosocial Roundtable, Breakthrough T1D has a path forward for tackling these pressing issues. We need to do more for the mental and emotional wellbeing of the T1D community—and we’re working hard to increase research into and awareness of psychosocial support programs that may improve the quality of life of people with T1D.
One way Breakthrough T1D is working to improve mental health care is through our recently launched Medical Affairs Program, which is addressing gaps between access to interventions and adoption by HCPs—a major effort that includes HCP education. It will be critical to integrate psychosocial care into clinician training and routine T1D visits.
Breakthrough T1D is also working to encourage innovative, interventional research and investing in promising studies—especially in less-studied areas, like T1D eating disorders. The next step is making sure that these studies can be incorporated into clinical practice by HCPs so they can be accessed by the people who need them most. We understand that psychosocial support needs to expand across the entire T1D population—including adults, people who are pregnant or recently diagnosed, and underserved communities—in order to have the greatest impact.
So, what can you do? Keep an eye out for psychosocial clinical trials that you or someone you know may be eligible to participate in. Refer to Breakthrough T1D’s mental health guide for additional support and guidance.
Breakthrough T1D strives to accelerate life-changing breakthroughs to cure, prevent, and better treat type 1 diabetes (T1D) and its complications. To accomplish these goals, we use a multi-pronged strategic approach, including conducting scientific studies and educating our community. In line with these goals, Breakthrough T1D recently published two peer-reviewed journal articles. One detailed burdensome unmet needs in the T1D community and identified key steps we can take to meet these needs. The other used real-world data to better understand American T1D demographics and predict changes in the next decade.
Let’s take a deeper dive into each.
Unmet needs of the T1D community: More work is needed
Despite major progress in T1D management, T1D still results in premature death, complications, and very significant daily burden.
Daily insulin use is a persistent challenge that comes with physical, emotional, social, and economic burdens.
New therapies and cures that can reduce or eliminate the challenges of living with T1D are closer than ever.
The entire T1D community (researchers, sponsors, clinicians, advocates, people with T1D, regulators) needs to work together to overcome scientific, drug development, and regulatory challenges to make cures for T1D a reality.
This commentary reviews previously existing data across the T1D care spectrum to help demonstrate the magnitude and significance of the unmet needs faced by people living with T1D. This information is used to emphasize the urgency researchers, sponsors, and regulators must place on developing cures for T1D. The authors provide recommendations and actionable steps to overcome scientific, clinical, and regulatory challenges that will help meet these needs.
Daily life with T1D is still a challenge
To say that the daily routine of people living with T1D is hard would be an understatement.
Insulin injections and dosage calculations. Wearable tech maintenance. Carbohydrate counting. Mealtime and exercise tracking. Doctor’s appointments. Hypoglycemia, hyperglycemia, and diabetic ketoacidosis (DKA) avoidance. It requires constant attention: 24 hours a day, 7 days a week.
The truth of the matter is that T1D management is a burdensome, demanding, and highly intensive task. There are no breaks, vacations, or time off—even overnight, it requires management. These challenges remain, even with today’s advancements in technology and the emergence of novel therapies for T1D. Simply put, we need to do more for the T1D community, and we cannot settle for the status quo.
The bigger picture
The global burden of T1D
11
The average number of years of life lost for people with T1D globally.
21%
The percent decrease in mortality rate for people with T1D in the last 30 years globally, which is not distributed equally among everyone with T1D.
The challenge of day-to-day T1D management compounds into long-term negative outcomes for the T1D population. Despite improvements in mortality rate, the life expectancy of people with T1D is still shorter than those without T1D.
Keeping blood glucose in a normal range is extremely difficult, and people with T1D need to be acutely aware of their insulin doses to prevent highs (hyperglycemia) and lows (hypoglycemia). Prolonged hyperglycemia leads to heart, kidney, and eye damage. Hypoglycemia can be very dangerous and a source of distress and anxiety, especially if it occurs often and eventually without symptoms (termed “hypoglycemia unawareness”).
The impact of hypoglycemia
25-40%
Percent of people with T1D who experience hypoglycemia unawareness.
30%
Percent of adults with T1D who have a fear of hypoglycemia.
Current technologies cannot solve the problem of hypoglycemia or make people with T1D have perfect blood sugar levels. As a whole, these challenges represent a profound emotional and mental burden for people with T1D, often leading to diabetes distress and burnout—which itself can lead to worse glycemic control. People with T1D have a tougher time managing the ins and outs of daily life because of the extreme mental and physical load of having T1D.
A longer life on its own is not the goal: it’s longer lives without ever having to think about T1D.
Breakthrough T1D’s vision for the future…
Breakthrough T1D envisions a world where the burden of T1D no longer exists. A world where people don’t have to manage their diabetes—they don’t take insulin, don’t have blood sugar highs and lows, and don’t develop complications. Curing T1D is our north star.
…and how to make it a reality
To achieve these goals, we need widespread screening, innovative research and therapies, patient-centered clinical approaches, and evolved regulatory pathways. We need to adjust the T1D paradigm and move clinical testing along at a quicker pace.
The regulatory route for new therapies determines whether companies, which have the greatest ability perform research in a quick and efficient manner, will invest their time and money into innovative T1D therapies. They are more encouraged to do so if they see defined and reasonable pathways for new therapies to reach the market—especially if healthcare systems are in place that will allow these therapies to be adopted by healthcare professionals and used by the people who need them most.
It starts with the decision-makers, who weigh the benefits versus risks of a new therapy. These decisions need to have more input from people who have a lived experience with T1D and can better decide if the benefits outweigh the risks, especially given the tremendous daily burden of living it. Clinical testing should broaden to include more populations of people with T1D—not just those who have severe disease—because nearly everyone has the chance to benefit. As the authors state in the commentary:
The magnitude of benefits required to outweigh a product’s risks should be determined by people living with T1D and no one else.
To further optimize T1D clinical trials, Breakthrough T1D and other experts have pushed for the validation of C-peptide, a biomarker for the body’s insulin production, as a clinical trial endpoint. Compared to the currently used endpoints, C-peptide would provide easier assessments and shorter clinical timeframes, thereby making the process of T1D therapy development more streamlined—and bringing these data to decision-makers sooner.
Once better clinical endpoints are validated, more personal experiences are incorporated into clinical trials, and the regulatory path to market is clear, companies will be encouraged to invest in T1D research programs, thereby speeding up research, innovation, and progress along the clinical pipeline—getting life-changing therapies into the hands people with T1D faster than ever.
What comes next?
This publication will be shared broadly with regulators, legislators, payers, and the T1D research community to encourage research, innovation, and funding and advocate for quicker, more efficient clinical testing and regulatory pathways to approval.
I think the misperception that the therapies available today are good enough is one of the most insidious challenges to ushering in the era of T1D cures…Today’s therapies do not offer the freedom from diabetes that people living with the disease want…I believe when we fully appreciate the daily experiences of people living with T1D, and when we use these experiences to guide our research development and regulatory decisions, we will also then have clear pathways for new therapies that meet these needs.”
Stephen Karpen, PharmDSenior Director of Regulatory Affairs at Breakthrough T1D
This is a call to action for everyone working in the T1D space. The overarching purpose is to foster awareness of these unmet needs and the urgency with which we must act as a community to address them—by working together and collaborating across the pipeline of T1D management.
Read on to learn more about the population of people living with T1D with these unmet needs.
Nearly 47% of Americans with T1D are enrolled in commercial health insurance followed by nearly 30% in Medicare, and 15% in Medicaid.
People with T1D who use diabetes devices have lower mortality rates than those who do not.
Most Americans living with T1D today are Non-Hispanic White people.
In the next 10 years, the Hispanic and African American populations with T1D are expected to grow the most, and the average age will increase from 47 to 49 years old.
The purpose of this study was to identify key T1D demographics in the United States and predict how these demographics will change over the next decade. Using healthcare insurance claim datasets, population growth projections, and existing literature, the authors modeled T1D demographic changes between 2024 and 2033.
This study was funded by Breakthrough T1D in collaboration with the T1D Index team so that these data can be incorporated into the Index. (Disclaimer: the T1D index uses multiple datasets and publications to predict the number of people living with T1D, which may explain discrepancies in Index estimates and predictions from this study).
Incidence
The number of new T1D diagnoses in a given time period.
Prevalence
The total number of people with T1D (new and existing diagnoses) in a given time period.
T1D stats: Now
2.07 million
Number of people in the U.S. living with T1D.
47
Average age of people living with T1D.
67%
Percent of people with T1D who are 20–64 years old.
19%
Percent of people with T1D who are over 65 years old.
47%
Percent of people with T1D who have commercial health insurance plans. Other coverage includes Medicare (30%) and Medicaid (15%).
T1D stats: 10 years from now
2.29 million
Number of people in the U.S. living with T1D (due to increase in T1D incidence and improved survival from devices).
49
Average age of people living with T1D.
33%
Percent increase in T1D population that aged 65 and older (mostly due to aging of the current T1D population).
38%
Percent increase in T1D population that is aged 10 and younger.
44%
Percent of people with T1D who have private/commercial health insurance plans. Other coverage includes Medicare (30%) and Medicaid (17.4%).
30%
Percent increase in T1D population who will use Medicaid.
What comes next?
Despite significant advances in T1D technology, therapies, and care management, the T1D population still faces a greater risk of complications and a higher mortality rate. Breakthrough T1D leadership will use key information from this study to inform future strategic research and advocacy efforts.
This data gives us an opportunity to quantify key information about our community to inform decision-makers…With better data specific to those with T1D, we can ensure that we’re advocating for solutions that not only expand access but also promote a better health care system for those with T1D.”
Lynn StarrChief Global Advocacy Officer at Breakthrough T1D
These data will help inform elected officials and payers about how healthcare policies may ultimately affect the T1D community—ensuring that the policies in place are having the greatest impact they can. The next phase of the project will analyze key demographic information in the context of access to cell therapies.
The ultimate goal is to ensure that everyone with T1D has access to the therapies, technology, and care that works best for them. By understanding T1D population demographics, Breakthrough T1D can make the most informed decisions possible as we move toward our goal of a world without T1D. We call on regulators, legislators, payers, and T1D researchers to take urgent action to meet the unmet needs of the T1D community now and in the future.
We value your privacy. When you visit BreakthroughT1D.org (and our family of websites), we use cookies to process your personal data in order to customize content and improve your site experience, provide social media features, analyze our traffic, and personalize advertising. By choosing “I Agree”, you understand and agree to Breakthrough T1D's Privacy Policy