Breakthrough T1D is focused on developing drugs, or disease-modifying therapies (DMTs), that change the course of T1D for everyone affected by it—and those yet to be. That means slowing or halting the progression of the disease, preventing it from ever occurring, and reversing it entirely through immune therapies and beta cell therapies.
Note: To enlarge the image below, left click on it.
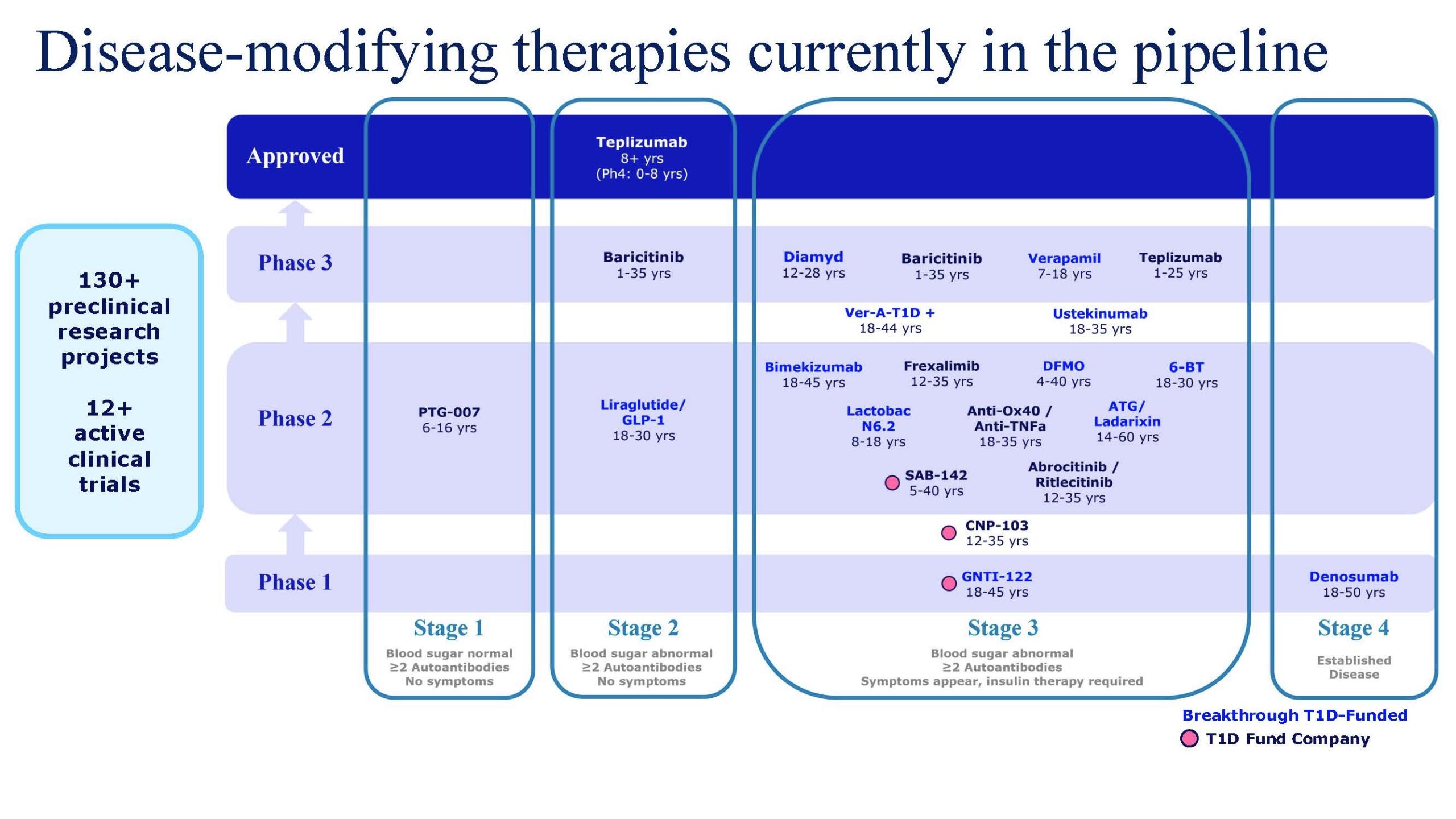
Update on Diamyd’s DIAGNODE-3 Clinical Trial
On March 27, Diamyd Medical announced results from an interim analysis of the Breakthrough T1D-funded Phase 3 DIAGNODE-3 trial, which assessed the ability of of Diamyd (retogatein or rhGAD65) to preserve insulin production (C-peptide) in the first 174 out of 321 participants in the trial.
Phase 3 Clinical Trials pave the way for discussions with regulatory agencies toward approval.
Surprisingly, and contradictory to positive data from prior phases of this clinical trial, the interim analysis showed that there was no observable preservation of insulin production (C-peptide). These results underscore the complexity of immune therapies in T1D and confirm Breakthrough T1D’s continued support of the clinical development of emerging disease-modifying therapies.
Breakthrough T1D’s Perspective on the DIAGNODE-3 Results
While this outcome was not expected, Phase 3 trials provide significant learnings for the development of future therapies and the field overall. Critical insight can be gained through the analysis of the data, even from clinical trials that do not meet their primary endpoint. These moments sharpen our understanding and accelerate better-designed approaches and more targeted application of therapies that are in development.
“Progress in type 1 diabetes research and treatment has always required persistence and learning from every study,” said Josh Vieth, Ph.D., Breakthrough T1D Senior Director of Research. “These results reinforce that immune interventions in type 1 diabetes are complex and highly context dependent. It’s imperative that we take these results seriously, understand what they mean, and use them to make strategic decisions about what’s next for retogatein and other disease-modifying therapies. There remains an unmet need for safe, effective therapies that rebalance the immune system in a targeted way, and Diamyd Medical is a pioneering approach to precision medicine for type 1 diabetes in clinical applications.”
What’s Next
Breakthrough T1D is in contact with the Diamyd team about next steps, which will include careful, collaborative analysis of the data from the trial to understand why these results differ from previous results. Diamyd plans to continue core operations, including manufacturing activities, during this period of analysis before determining the appropriate course of action. This includes the possibility of testing this therapy earlier in the progression of T1D (Stage 1 or 2), for which they have previously received “Fast Track” designation, an FDA program which would expedite this process.
Our Multi-part Strategy for Disease Modifying Therapy Development
Breakthrough T1D has been funding DMT research for decades. Following the 2022 approval of Tzield, the first DMT for T1D, we remain focused on our strategy for the development of disease-modifying therapies that can slow, halt, or reverse the course of T1D.
This strategy aims to both rebalance the immune attack as well as support a person’s own beta cells. Tolerization, or re-training the immune system to stop attacking beta cells without broad immunosuppression is an important part of that strategy. We are currently funding disease-modifying trials with companies like GentiBio to test their engineered Tregs, and trials aimed at repurposing existing drugs including DFMO, Bimekizumab, Denosumab, and ATG for use in T1D. To learn more, consult our previous article about this work.
November 2022 was a historic moment for the type 1 diabetes (T1D) community: Teplizumab (Tzield), the first disease-modifying therapy (DMT) for T1D, was approved by the FDA.
Tzield has been game-changing for T1D. It’s the first therapy for the disease that addresses the root cause of T1D, not the symptoms. It targets the T cells that are responsible for destroying insulin-producing beta cells, slowing down the autoimmune processes that cause T1D. Tzield has proven to delay progression to Stage 3 T1D—when insulin therapy is often required—for up to three years.
The approval of Tzield was a culmination of decades of passionate work by Breakthrough T1D, the only organization that supports T1D therapy development at every stage—from discovery research all the way through to people with type 1 diabetes receiving these therapies with healthcare coverage paying for them.
Pioneering Research and Strategic Investments
In the late 1980s, Kevan Herold, M.D., had just started his faculty-level career at The University of Chicago. He was diagnosed with T1D several years earlier, which heavily influenced his decision to focus on endocrinology. There, he met Jeff Bluestone, Ph.D., an immunologist concentrating on cancer research. After meeting many members of the T1D community through Dr. Herold, Dr. Bluestone switched a large portion of his research to new therapies for T1D.
One of their early studies showed that type 1 diabetes onset could be delayed with an anti-CD3 antibody, which later became teplizumab. Breakthrough T1D supported this novel research, which led to the first-ever clinical trial of a T1D disease-modifying therapy in humans in the early 2000s. The trial was a success and laid the groundwork for further studies and eventual support from the National Institutes of Health (NIH) through the Special Diabetes Program (SDP).
Over the next two decades, teplizumab was acquired by MacroGenics, a company formed to develop immune-based therapeutics for autoimmune diseases and cancer, then sold to Provention Bio, a T1D Fund-backed biopharmaceutical company focused on disease interception and prevention. The drug underwent several NIH and Breakthrough T1D-funded clinical trials; it was Provention Bio’s PROTECT trial that pushed it over the finish line to FDA approval in 2022.
In 2023, Provention Bio was acquired by Sanofi. This brought the first T1D disease-modifying therapy into the portfolio of a leading global pharmaceutical company. It also represented a significant endorsement of the potential of DMTs to have an impact on people living with T1D.
People like Chris Dunn.
Breakthroughs in Action
Chris Dunn is a parent of four children, two of whom live with T1D. Knowing that immediate family connections are a risk factor for developing T1D, Chris and her children without T1D participated in screening.
Much to her surprise, Chris’ screening results revealed the presence of multiple T1D antibodies; further testing indicated she was in stage 2. Chris knew that Tzield could potentially delay her need for insulin therapy, so she made the informed decision to undergo treatment.
“I’ve had a front row seat to this disease for nearly 20 years,” Chris said. “Any day that you can save yourself from having to be on insulin therapy and all of the risks that come with that is worth it to me.”
Chris represents our research breakthroughs in action. She hopes that Tzield will delay the onset of Stage 3 T1D until cell therapies are available to cure the disease.
The Future of Tzield
As Tzield becomes more widely used in people over the age of 8 in Stage 2 type 1 diabetes, Breakthrough T1D’s Disease-Modifying Therapies Program is exploring how it may benefit other ages and stages.
“We continue to fund research to discover and develop new interventions and new ways of rebalancing the immune system, ultimately working toward our goal of a world without type 1 diabetes,” said Joshua Vieth, Ph.D., Senior Director of Research at Breakthrough T1D.
In October 2025, Tzield was accepted into the FDA Commissioner’s National Priority Voucher program for accelerated review. If approved, this could lead to expanded use of Tzield for people with newly diagnosed Stage 3 T1D (when insulin therapy is required). This is significant—it would be the first time people at this stage could have the option for a disease-modifying therapy.
Delaying the onset of T1D in young children would be transformative for families facing a diagnosis. Interim results from an ongoing clinical trial, PETITE-T1D, showed that Tzield is safe and well-tolerated in children under 8 with Stage 2 T1D. Final results of the study are expected sometime this year, and Tzield has been accepted for priority review by the FDA for this population.
While Tzield is the first approved disease-modifying therapy for T1D, Breakthrough T1D will make sure it’s not the last. Our goal is to not just delay T1D progression but stop it entirely, or even reverse its course. We will support the continuous development of these therapies to change the trajectory of type 1 diabetes for everyone affected by it—and those yet to be—to cure the disease.
Closing the gap between access to and adoption of type 1 diabetes (T1D) therapies is a mission priority for Breakthrough T1D.
Our newly created Medical Affairs unit provides education and resources for the entire T1D community, from clinicians to people living with the condition, so that everyone impacted by T1D is empowered to make informed decisions about healthcare and emerging therapies.
Chris Dunn represents our efforts in action.

Chris is a parent to four children, two of whom live with T1D. Knowing the increased risk of T1D in immediate family members, Chris and her children without T1D participated in screening. In what she could only describe as “surreal,” Chris’ screening results revealed the presence of multiple T1D antibodies; further testing indicated she was in stage 2.
For decades, Breakthrough T1D funded discovery research, supported clinical development, and worked with regulators to bring Tzield—the first disease-modifying therapy for type 1 diabetes—to market. Tzield is available to people in stage 2 type 1 diabetes—like Chris—and can delay progression to stage 3, or clinical onset of T1D, for up to three years. This means potentially years without blood-sugar monitoring, insulin administration, and the fear of short- and long-term complications.
Watch Chris’s story now:
Part 1: Screening and Early Detection
Part 2: Early Detection and Disease-Modifying Therapies
Type 1 diabetes (T1D) doesn’t discriminate. It affects people of all races, ethnicities, ages, and socioeconomic backgrounds. Although its exact causes are unknown, researchers have uncovered type 1 diabetes risk factors that increase a person’s likelihood of developing the condition.
Family history
Having a family history of type 1 diabetes is the highest risk factor for developing the disease—a first-degree relative (parent, sibling, or child) with T1D increases your risk up to 15-fold. However, nearly 85% of diagnoses occur in people who have no family members with the disease.
Breakthrough T1D-funded researchers have tracked data from nearly 8,000 high-risk children to estimate future risk for T1D more precisely in The Environmental Determinants of Diabetes in the Young (TEDDY) study. A family follow-up to this study focuses on screening and monitoring siblings and parents of TEDDY participants, who have an increased genetic risk for T1D. The goal is to enhance early detection and prevention programs, better understand the natural progression of T1D, and potentially identify new genetic markers that can help predict the risk of T1D development.
Early Detection
Thanks to advances in research and a better understanding of the human immune system, we are now able to identify a person’s risk for T1D many years before the onset of symptoms through a simple blood test. Screening can reduce the risk of complications at diagnosis and also help researchers better identify who is at risk. This leads to the development of disease-modifying therapies that can slow, halt, or reverse the progression of T1D.
Age
A person’s age is a type 1 diabetes risk factor. While people can experience the onset of T1D at any age, many are diagnosed in early elementary school or as preteens, with ages 10-14 having the highest occurrence of diagnoses.
Environmental triggers
Research has not found a definite environmental trigger for type 1 diabetes. Viruses and exposure to gluten, cow’s milk, antibiotics, and more have all been extensively studied, yet no certain links have been made. “The evidence has not been conclusive,” says Laura Jacobsen, M.D., Assistant Professor and Pediatric Endocrinologist at the University of Florida. “It may be because there are multiple or different triggers for different subsets of the population.”
Ethnic and geographic triggers
The risk for type 1 diabetes has historically been highest in those with white European ancestry. However, the diversity of the population with T1D is increasing, meaning the risk is going up in minority populations. Research is ongoing in this area to address this increasingly global problem. Visit the T1D Index for a detailed look at type 1 diabetes prevalence around the world.
Geographically, there are countries where the risk of T1D is higher than others, but “ultimately it is underlying genetics that impact risk,” Dr. Jacobsen said.
Researchers are still trying to understand how and why genes and environment are T1D risk factors. Breakthrough T1D continues to fund this research so that, one day, we will be able to prevent, reverse, and cure type 1 diabetes.
ADA Recap Series
This article is the second of our three-part ADA Recap Series. Breakthrough T1D was on site in Chicago, IL from June 20-23 for the American Diabetes Association’s (ADA) 85th Scientific Sessions. We’re here to report on the latest-and-greatest type 1 diabetes (T1D) advancements—including many driven by Breakthrough T1D funding. Look out for tomorrow’s article for updates on Medical Affairs.
Cures
Breakthrough T1D’s Cures program focuses on early detection, disease-modifying therapies, and cell therapies with the goal of working toward effective cures for T1D.
Cell therapies were front-and-center at ADA 2025. We have some exciting clinical trial updates and new ideas for optimizing islet transplantation.
Cell therapies
Autologous cell transplantation
Autologous cells are those removed from an individual and implanted back into the same individual. These cells can be modified in a laboratory before implantation. Autologous cells are still susceptible to autoimmunity in T1D, so cell protection strategies (gene-editing, encapsulation, immune modulation, etc.) are expected to be required.
Allogenic cell transplantation
Allogenic cells are those that are derived from a source other than the recipient, such as deceased donors or precursor-derived manufactured cells. Allogenic cell transplants require immunosuppression because they stimulate an immune response. Breakthrough T1D’s Cell Therapies program is focused on allogenic cells—specifically manufactured cells—because they can be generated at large scale.
One-year updates on Vertex’s manufactured cell therapy, zimislecel
- Presenter: Michael Rickels, M.D. (University of Pennsylvania)
- Zimislecel (VX-880) is a manufactured islet therapy that requires immunosuppression, infused into a vein in the liver in people with T1D who have impaired hypoglycemic awareness and severe hypoglycemic events.
- The phase 1/2 clinical trial, which is part of the pivotal phase 1/2/3 FORWARD-101 trial, is complete. Twelve participants received a single infusion of a full dose of cells and were followed for at least one year.
- All 12 participants achieved the primary endpoint, which was elimination of severe hypoglycemic events and HbA1c levels less than 7%. 10/12 (83%) participants are insulin independent.
- All 12 participants demonstrated sustained insulin production as measured by C-peptide, reduced external insulin therapy use, and achieved greater than 70% time in range.
- There were no serious adverse events. Mild to moderate adverse events were consistent with the immunosuppression regimen, infusion procedure, and complications from T1D.
- These data were published in the New England Journal of Medicine and represent further evidence of the curative potential of manufactured islet transplantation for T1D.
- Breakthrough T1D’s support for Doug Melton, Ph.D.—whose proprietary lab-created beta cells are now being advanced by Vertex—goes back decades, both via research grants and an investment from the T1D Fund: A Breakthrough T1D Venture.
6-month update on Sana Biotechnology’s immune-evasive islets
- Presenter: Per-Ola Carlsson, M.D., Ph.D. (Uppsala University)
- Sana’s donor-derived islet therapy engineered with Hypoimmune (HIP) technology can evade the immune system without immunosuppression.
- These cells were implanted intramuscularly in a first-in-human study into a person with T1D with no measurable insulin production.
- Six months post-transplant, this person is consistently making their own insulin, as measured by C-peptide levels. Yet, they still require external insulin therapy because they received a smaller dose of cells than the dose that would be required to achieve insulin independence. They did not experience any serious side effects, so the cells and procedure are safe and well-tolerated.
- A Mixed Meal Tolerance Test (MMTT) confirmed that these cells are not only surviving but also responding to changes in blood glucose levels.
- This is a promising first step toward a functional cure for T1D that does not require immunosuppression. Sana Biotechnology is planning on applying this technology to manufactured islets.
- Sana has received support from the T1D Fund to advance their HIP technology in islets, and Breakthrough T1D continues to work closely with them.
A new transplantation site for autologous manufactured islets
- Presenter: Hongkui Deng, M.D. (Peking University)
- Cells derived from adipose tissue (fat) can be removed from a person and chemically induced in the laboratory to become islet cells.
- Implantation of autologous manufactured islets into the sub-anterior rectus sheath in preclinical models of T1D improves glycemic control.
- In humans, this implantation site is easily accessible by an ultrasound-guided needle.
- In a first-in-human study, autologous manufactured islets were implanted into this site in a person with T1D. This person no longer needs external insulin therapy and has greatly improved blood glucose control. This person had also received a liver transplant and was taking immunosuppressants.
A new encapsulation device for immune protection of transplanted islets
- Presenter: Nicolas Laurent, Ph.D. (Adocia)
- Adoshell® is a novel islet cell encapsulation device that can shield islets from the immune system, meaning that immunosuppressants are not needed.
- The hydrogel-based device is non-degradable, easily retrievable, and allows the exchange of glucose and insulin from the vasculature surrounding the device while excluding immune cells from encapsulated islets based on pore size.
- This device showed promise in animal models, and human clinical testing is next.

Cell therapies highlight: Breakthrough T1D-funded research
Tom Bollenbach, Ph.D. (Advanced Regenerative Manufacturing Institute; ARMI) presented on challenges and solutions for large-scale manufacturing of islet cells. The goal is to generate scalable, automated manufactured islets that can be used by labs around the world to accelerate research progress using a unique, validated, and reliable cell source. Some challenges include ensuring the manufactured cells can survive shipment from the facility to research labs and maintain their insulin-producing capacity when they are used in different labs. ARMI is working with the Beta Cell Replacement Consortium to address these challenges.
Antonio Citro, Ph.D. (San Raffaele Hospital) presented his work on ensuring that transplanted islets have enough oxygen and nutrients (“vascularization”) to survive and function. Dr. Citro described an approach tested in animal models referred to as “natural scaffolds” in which all cells are removed from a donor organ, such as a lung, leaving behind blood vessel structures and other structural components. Islet cells can be injected and grafted onto this scaffold to create a mini organ of islet cells, which can then be tested for functionality before and after implantation.
Andrew Pepper, Ph.D. (University of Alberta) also presented vascularization strategies to increase the survival and functionality of transplanted islets. The implantation of a biomaterial under the skin will trigger the immune system and initiate a foreign body reaction, which results in the formation of blood vessels and structural components around the foreign object. Removal of the object leaves a hollow pre-vascularized core suitable for islet transplantation. This process can be optimized by using a biodegradable material, so no removal is required, and by the addition of “accessory cells” that help maintain a vascularized environment for islets.
Key takeaways
Cell therapies are making significant headway in clinical trials, and people receiving manufactured cells are becoming insulin independent. Researchers are tackling the biggest challenges for optimizing islet transplantation, including large-scale manufacturing, ensuring cell survival, and preventing detection by the immune system.
Disease-modifying therapies
A major focus at ADA 2025 was addressing the underlying immune mechanisms of T1D—including alterations in immune cells that facilitate beta cell destruction and other factors that contribute to autoimmunity onset. Read on for some highlights.
The role of B cells in T1D autoimmunity
- Presenter: Mia Smith, Ph.D., DVM (University of Colorado)
- B cells are a type of immune cell that can activate destructive immune cells that facilitate autoimmunity in T1D.
- B cells can become wrongly activated against insulin-producing beta cells due to converging dysregulation of factors that regulate immunity.
- These cells represent another potential target for disease-modifying therapies in T1D.
Disease-modifying therapies highlight: Breakthrough T1D-funded research
Emrah Altindis, Ph.D. (Boston College) presented on the role of the gut microbiome in T1D. His studies found that people with T1D tend to have more inflammatory bacteria in their gut microbiome. Dr. Altindis and his team identified a particular bacterial population that can enhance T1D onset in animal models due to changes in immune cells that contribute to T1D autoimmunity. These studies provide insight into additional factors that can drive immune changes in T1D.
Laura Sanz Villanueva, MSc (St. Vincent’s Institute of Medical Research), who works in the lab of Breakthrough T1D-funded researcher Professor Thomas Kay, MBBS, Ph.D., presented on a mechanistic follow-up study to the BANDIT clinical trial. The Breakthrough T1D-funded phase 2 BANDIT study showed that baricitinib, a JAK1/2 inhibitor that prevents immune cell communication, can increase insulin production as measured by C-peptide in people with recently diagnosed T1D. The present study found that baricitinib can reduce the number of natural killer (NK) cells in the pancreas, which are involved in the autoimmune destruction of beta cells. These data provide valuable insight into the mechanism of baricitinib-mediated protection of beta cells.
Key takeaways
T1D is driven by dysregulation of the immune system, which results in an attack on insulin-producing beta cells. Researchers at ADA 2025 spoked about novel factors—including B cells, NK cells, and T1D autoimmunity triggers—that may contribute to immune cell dysfunction in T1D.
Early detection
A key focus at ADA 2025 was the growing recognition of the heterogeneity of T1D, including autoantibody-negative disease onset, genetic variation, and the frequent misdiagnosis of T1D in adults, underscoring the need for greater diversity and inclusion in research and care. The expanded role of continuous glucose monitoring (CGM) and continuous ketone monitoring (CKM) was also highlighted, not only for daily management but as essential tools for understanding disease progression.
Using genetics to predict T1D risk
- Presenters: Richard Oram, M.D., Ph.D. (University of Exeter), Leslie Lange, Ph.D. (University of Colorado), Aaron Deutsch, M.D. (Massachusetts General Hospital), Josep Mercader, Ph.D.(Massachusetts General Hospital) and Eimear Kenny, Ph.D. (Icahn School of Medicine at Mount Sinai)
- Polygenic risk scores (PRS) estimate the risk a person has for developing a disease like T1D based on variations in different genes.
- Ancestry is a major influence on PRS, particularly based on differences in genes that regulate whether the immune system can distinguish between “self” and “non-self.”
- Most PRS models have been developed using data from European populations and have a limited ability to accurately determine risk in other ethnic groups, such as individuals of African and East Asian descent.
- Potential applications of PRS include incorporation into screening to better understand T1D risk, ensure accuracy in diagnostic tests, and develop precision medicine-based therapeutic approaches.
Understanding how genetic diversity contributes to T1D
- Presenters: Suna Onengut-Gumuscu, Ph.D. (University of Virginia), Dominika A. Michalek, MS (University of Virginia), Aaron Deutsch, M.D. (Massachusetts General Hospital), and Stephen I Stone, M.D. (Washington University School of Medicine), among others.
- These talks highlighted several studies conducted in diverse populations to better understand the pathophysiology of T1D.
- Work presented from Consortia, such as RADIANT, focused on rare and atypical forms of diabetes.
Controversies in CGM and benefits for early detection
- Presenters: Peter Calhoun, Ph.D. (Jaeb Center for Health Research), Michael Kohn, M.D., MPP (University of California San Francisco), Nicole Ehrhardt, M.D. (University of Washington) and Tadej Battelino, M.D., Ph.D. (University of Ljubljana)
- CGM use holds value in identifying progression in early stages of T1D prior to symptomatic onset.
- There was a call to update the clinical guidelines so that the benefits of CGM can be maximized within the T1D community—including at early and later stages of T1D.
- Integrating newer measures of blood glucose, like the glucose management indicator (GMI) and time in tight range (TITR), will be essential.
Contributions of CKM to early detection
- Presenters: Ketan Dhatariya, MBBS, M.D., Ph.D. (Norfolk and Norwich University Hospitals), Lori Laffel, M.D., MPH (Harvard University), Jennifer Sherr, M.D., Ph.D. (Yale University), and Richard Bergenstal, M.D. (HealthPartners Institute).
- It will be critical to explore whether ketone monitoring could help reduce the incidence of diabetic ketoacidosis (DKA) at stage 3 clinical T1D onset.
- Early detection of rising ketones will be important for people with T1D to take action before DKA occurs.
Early detection highlight: Breakthrough T1D-funded research and awardees
Brigitte Frohnert, M.D., Ph.D. (Barbara Davis Center for Diabetes), co-investigator with Breakthrough T1D-funded researcher Andrea Steck, M.D., presented on the evolution of CGM patterns prior to stage 3 T1D. Their longitudinal approach, with CGM data collected at three-month intervals, successfully distinguished individuals who progressed to stage 3 T1D clinical onset from those who did not. This research suggests that CGM may be beneficial for predicting clinical progression of T1D.
Anette-Gabriele Ziegler, M.D. (Helmholtz Munich) was awarded the Harold Hamm Prize for Biomedical Research in Diabetes 2025, highlighting her important contributions on T1D screening in the pediatric population.
Barbara B Kahn, M.D. (Beth Israel Deaconess Medical Center and Harvard Medical School) received the 2025 Albert Renold Award, and her role model for women in science was highlighted at the Women’s Interprofessional Network of the ADA (WIN ADA).
Key takeaways
T1D arises in diverse ways across age groups and ancestries, complicating diagnosis and treatment. At ADA 2025, experts highlighted how genetic and clinical heterogeneity demands more inclusive strategies. Tools like CGM and CKM were highlighted for their potential to enhance clinical management in the early stages of T1D.
Breakthrough T1D’s Cures team making an impact
Sanjoy Dutta, Ph.D., Chief Scientific Officer, participated in a panel discussion titled “Encapsulation vs. Naked Cell Therapy—Immune Challenges and Beta-Cell Perspectives in Diabetes Treatment.” The panelists covered different approaches to preventing immune attack of transplanted islets, including gene-editing, in addition to pros and cons of different transplantation sites.
Esther Latres, Ph.D., Vice President of Research, and Jay Tinklepaugh, Ph.D., Senior Scientist, hosted a workshop immediately after ADA titled “Islet Cells in T1D.” Breakthrough T1D-funded researchers gathered from around the world to discuss cell therapy clinical trial updates, mechanistic insights into islet function, targeted delivery of therapeutics to beta cells, and optimization strategies for islet transplantation.
Look out for tomorrow’s article for an update on Medical Affairs presented at ADA 2025!
Photo Credit: USGA/Jason E. Miczek
J.J. Spaun drew cheers from golf fans and people with type 1 diabetes (T1D) alike with his unbelievable 64-foot birdie putt on the final hole to win the 125th U.S. Open at Oakmont in Pennsylvania. Spaun’s strong performance throughout the 2025 PGA Tour season also qualified him for his first U.S. Ryder Cup, where he will join Xander Schauffele and Scottie Scheffler as part of the U.S. team.
While his rally and wins are an amazing, once-in-a-lifetime experience—and exemplify how people with T1D can accomplish anything—his diagnosis with T1D as an adult, which he has shared publicly, was unfortunately all too common: he was first classified as having type 2 diabetes (T2D).
This led to challenges, including more weight loss, a calorie-restricted diet, and side effects from blood-glucose levels that remained stubbornly less-than-optimal. Eventually, his golf game was affected. Then, he saw a specialist, who correctly diagnosed him with T1D.
In a 2022 Golf Channel web story about the situation, Spaun said, “I went through two years of struggling. I’m not blaming that, but that was another contributing factor. I was doing the wrong things. The regimen for type 2 is a little different than for a type 1; I’m not even getting the right medicine to regulate my blood sugar. … I was eating nothing, probably less than 1,500 calories a day, and still having high glucose side effects as a ‘type 2,’ so that’s why I needed the insulin to help level that out and be able to eat more calories in general.”
Recognizing type 1 diabetes in adults
As evidenced by Spaun and other adults diagnosed with type 1 diabetes, the condition can strike anyone at any age. The idea that T1D is only diagnosed in children is antiquated and inaccurate, yet adults with T1D continue to be misclassified as having T2D. According to an article published in the journal The Lancet, Regional Health: Europe, it is estimated that nearly 40 percent of adults older than age 30 with T1D may have been misclassified as having T2D, which is far more prevalent in adults than T1D. Additionally, 37% of type 1 diabetes diagnoses in the United States occur after age 30, states a 2023 article published in the journal, Annals of Internal Medicine.
A simple blood test can detect T1D in the earlier stages. The biggest challenge is educating clinicians and the general population about it.
Endocrinologists, pediatricians, and some other specialty physicians learn about T1D screening and monitoring during their residencies, but it’s not a part of the general curriculum of the first four years of medical school. As such, many healthcare professionals know to order an HbA1c test for T2D but do not know what test to order for T1D. In addition, many clinicians understandably hesitate to order unfamiliar tests—especially if they are unsure what to do with the results.
Screening and monitoring for more accurate diagnoses
Breakthrough T1D’s new healthcare professional resources aim to advance the knowledge of T1D screening and monitoring to clinicians whose patients could most benefit from it, which turns out to be just about everyone. According to a paper published in the journal US Endocrinology, roughly 85 percent of people diagnosed with type 1 diabetes do not have a blood relative with the autoimmune disease.
Spaun’s experience and the experiences of all adults with type 1 diabetes who were first classified as having T2D point to the importance of T1D screening and monitoring for accurate diagnoses in people of all ages.
Learn more
Knowing if you have type 1 diabetes autoantibodies gives you options. Detect so you can decide.
Learn about options for getting screened and what to do with results if you or a loved one have positive screening results.
Learn more about type 1 diabetes, including how it differs from other kinds of diabetes.
Learn more about our accredited education and type 1 diabetes educational resources for healthcare professionals.

When Tzield was approved by the United States Food and Drug Administration (FDA), the type 1 diabetes (T1D) community had real cause to celebrate: The first disease-modifying therapy for T1D had cleared one of the last major hurdles to becoming available.
Disease-modifying therapies
Also "DMTs" for short, these therapies prevent, slow, halt, or reverse T1D progression.
But once Tzield was on the market and covered by health insurance companies and other payers, a new hurdle emerged: a majority of healthcare providers across the country were unaware of the drug, let alone how to administer it.
The clinical guideline for Tzield infusion did not become available until a year and a half after the FDA approved the drug. To date, 500 people in the U.S. with early stage T1D have received Tzield. Compare that to the annual incidence rate of T1D in the U.S. according to the T1D Index:
52,560
Number of people in the U.S. diagnosed with type 1 diabetes annually.
According to a 2023 study in the journal Diabetes Technology & Therapeutics, Tzield isn’t the only advanced T1D therapy with a surprisingly low adoption rate.
The FDA approved the first artificial pancreas (AP) system in 2016. Less than a decade later, there are now eight such approved systems on the market. These systems—also called automated insulin delivery (AID) systems—lead to better T1D management and health outcomes—yet only 16 percent of people with T1D in the United States use them.
Similarly, the FDA approved Lantidra, the first donor-derived cell therapy for T1D, in 2023. To date, one person has received it.
Increasing adoption to improve health
Closing the gap between access to and adoption of T1D therapies is a mission priority for Breakthrough T1D.
“It’s similar to the question: ‘If a tree falls in the forest and no one is there, does it make a sound?’” said Anastasia Albanese-O’Neill, Ph.D., APRN, CDCES, Associate Vice President of Breakthrough T1D’s Community Screening and Clinical Trial Education programs. “In this case, if you have a cutting-edge new therapy but most healthcare providers don’t know about it, don’t prescribe it, and don’t know how to administer it, does it have an impact?”
The organization recently announced the establishment of a Medical Affairs unit. The team will address the numerous challenges contributing to the slow adoption of groundbreaking T1D therapies, delaying their life-changing potential for many people living with the disease.
Challenges we are addressing:
HCPs have much greater knowledge of type 2 diabetes—or T2D—which is more prevalent.
HCPs need comprehensive guidelines to support new, approved treatment options.
There are too few clinical environments with the equipment and expertise to administer advanced T1D therapies and treatments, such as new T1D devices, therapies that require infusions like Tzield, and treatments that require implantation, such as cell therapies.
There are too few endocrinologists and certified diabetes care and education specialists with knowledge and competency in advanced T1D therapies.

With the establishment of our Medical Affairs team, we are reaffirming our organization’s commitment to creating a world where every individual with type 1 diabetes has access to life-changing therapies. By addressing systemic barriers and fostering clinical readiness, Breakthrough T1D will be pivotal in driving the timely adoption of emerging therapies and transforming care.”
As part of this organizational change, the Community Screening and Clinical Trial Education team, led by Albanese-O’Neill, will be integrated into Medical Affairs.
The team will focus on developing education materials for healthcare professionals in the U.S. and around the world; empowering people with T1D to participate in shared decision-making with their healthcare teams about emerging T1D therapies; helping to establish and socialize clinical care guidelines tailored to regional needs; and expanding clinical trial participation through community activation and HCP education.
“We have been doing a great deal of work to expand our HCP education, T1D community screening, and clinical trial education programs for more than three years now,” said Albanese-O’Neill, who has been with Breakthrough T1D as a fulltime staff member since 2022. “Given what we are seeing with adoption rates and with Dr. Danne joining us, we are now putting all of this work together in one department with a more strategic approach.”

Empowering clinicians with education
The team recently launched comprehensive, expertly redesigned HCP education and training resources.
These resources—which are accredited, free-of-charge, and live or on-demand—offer a significant focus on early detection for the earliest stages of T1D, monitoring guidance for positive test results, clinical trial opportunities, and the latest on cutting edge T1D therapy research and development, including disease-modifying therapies and islet cell therapies.
While designed specifically for healthcare professionals who can earn 4.5 credit hours of continuing medical education, the resources are available to the public. The on-demand feature means busy healthcare professionals with schedules that include all kinds of shifts imaginable can access this turn-key resource on their own time.
For a deeper dive, Breakthrough T1D’s resources will also offer live sessions, allowing time to interact with and learn from leading experts in the T1D field, including Albanese-O’Neill and Danne, in addition to those affiliated with different clinical facilities and institutions across the nation.
Our goal is to make this education as accessible as possible.”
Detecting T1D before symptoms present
A simple blood test can detect T1D in the earlier stages—before obvious symptoms develop. The biggest challenge is educating clinicians and the general population about it.
“Endocrinologists, Pediatricians, and some other specialty physicians learn about T1D screening and monitoring during their residencies, but it’s not a part of the general curriculum of the first four years of medical school,” said Lally, who built the learning management system for the new resources and is organizing the virtual offerings. “We’re working to advance that knowledge to yes, doctors, but also other clinicians whose patients could benefit.”
Many clinicians hesitate to order unfamiliar tests—especially if they are unsure what to do with the results. Most people who see any kind of healthcare provider could benefit from screening for T1D—according to a paper published in the journal US Endocrinology, roughly 85 percent of people diagnosed with type 1 do not have a blood relative with the autoimmune disease.
“Clinicians need to learn about the stages of type 1 and the specific autoantibody tests that identify type 1 versus type 2 and identifying type 1 in individuals at risk before they need insulin,” said Colleen Buggs-Saxton, M.D. Ph.D.
Buggs-Saxton, a Pediatric Endocrinologist at Wayne Pediatrics in Michigan, is the clinical leader of a Breakthrough T1D Early Detection pilot clinic. Using the new resources, she and Albanese-O’Neill are going to lead a grand rounds about T1D early detection at her institution, which is affiliated with the Wayne State University School of Medicine and healthcare system.

Clinicians should consider autoantibody testing for adults who have been diagnosed with type 2 but don’t have typical clinical features and require insulin to manage their blood sugars.”
“This is a novel way these resources can be used—as the basis of a locally and or virtually-provided grand rounds,” said Albanese-O’Neill.
While much of the emphasis of T1D early detection programs has been on children and teens, its applications are much broader—anyone can develop T1D at any age and unfortunately, misdiagnoses happen. According to an article published in the journal The Lancet, Regional Health: Europe, it is estimated that nearly 40 percent of adults older than age 30 with T1D may have been misdiagnosed with T2D.
“Most clinicians are very comfortable ordering an HbA1c test to classify people with type 2 diabetes, but they do not know what tests to order to classify people with type 1,” added Buggs-Saxton.
Grand rounds
Grand rounds are educational meetings and presentations for clinical teams at a given institution or healthcare facility to provide a summary of updates to the standards of care.
What to do with positive test results
The screening test is just the first part of T1D early detection. Clinicians also need to know what to do with positive results once they come in. Breakthrough T1D’s HCP resources offer extensive education on the topic.
Less than one year ago, Breakthrough T1D and other leading diabetes organizations developed monitoring guidance to help clinicians support people who test positive for stage 1 or stage 2 T1D. The guidelines have been endorsed by leading medical journals and organizations around the world.
”This monitoring guidance can help any clinician feel confident in providing adequate care in the early stages of type 1 and know when to refer to a specialist,” said Albanese-O’Neill.

I think of research, advocacy, and medical affairs as three legs of a stool—in terms of clinical adoption, each helps answer a different question. Research: Does it work? Advocacy: Will the regulators approve it and will insurance companies cover it? Medical Affairs: Do clinical teams have the competency and readiness to prescribe the treatment and educate and support people with T1D?”
It’s also helpful for the people who test positive for early stage T1D. Using the monitoring guidance, people can work with their healthcare team to monitor blood glucose levels to identify when insulin therapy may be needed; consider participating in clinical trials of disease-modifying therapies in development; and consider when and whether Tzield might be appropriate.
“There is currently one FDA-approved disease-modifying therapy for early-stage type 1 diabetes and additional therapies are being studied in clinical trials,” said Lally. “Identifying type 1 early gives the individual and their family time to learn more about type 1 and their options before reaching stage 3 T1D, which requires daily insulin therapy.”

Clinical trials: Increasing patient referrals
Clinical trials are a vital step for any treatment, drug, or device to make it into the hands of people with T1D. Currently, more than 300 clinical trials focused on T1D are actively recruiting participants.
Moreover, clinical trials can offer people the chance of receiving a cutting-edge treatment they may not otherwise be able to access.
Through its HCP resources and existing clinical trial resources, Breakthrough T1D is stressing the significance of investigational T1D therapies—while also clarifying common misconceptions about clinical trials.
“The clinical trial education portion of the program explains current trial opportunities and the critical need to increase diversity in diabetes research,” said Lally.
Despite the importance of clinical trials, many are delayed due to slow enrollment, adding cost and prolonging the results. A 2020 Tufts University study found that nearly 90 percent of clinicians surveyed felt comfortable talking about clinical trials.
“Unfortunately, the survey also revealed that annually, fewer than one percent of patients are referred to clinical trials,” said Lally.
So, why aren’t more clinicians referring their patients to clinical trials? Time and resources.
The most challenging part is helping patients understand what a clinical trial is, what it involves, and how previous scientific advances were only possible because of clinical trials. Healthcare providers often don’t have enough time in their busy clinics to discuss this with patients and families.”
Jacobsen, who is with University of Florida Health (UF Health), is one of the faculty members for Breakthrough T1D’s new HCP resources—specifically, the offering related to currently recruiting clinical trials for T1D disease-modifying therapies.
Jacobsen stresses that families and individuals with T1D also need specific education on the potential of receiving a placebo during a clinical trial—and why it’s an impactful part of any clinical trial.
Clinicians also may not know how to quickly get and stay up to date on current trial opportunities and how to get individuals who test positive for T1D autoantibodies involved.
“We provide a streamlined presentation about how to talk to families of people with T1D or people at risk for T1D about clinical trials,” explains Jacobsen, “We can direct families to one of several websites for more detailed information, like Breakthrough T1D’s Clinical Trial Finder.”

Cell therapies: Cures within reach
Cell therapies are one of the most promising approaches to curing T1D and one of the cornerstones of Breakthrough T1D’s cures research portfolio.
Advances in cell therapies have ramped up in recent years: participants in clinical trials of these therapies have been able to stop taking insulin. To speed this progress even more, Breakthrough T1D recently launched Project ACT (Accelerate Cell Therapies).
Cell Therapies
Also called islet cell therapies, these therapies replace destroyed beta cells so that people with T1D can again produce their own insulin.
The organization has long invested in cell therapy research and has a track record of success in making life-changing T1D therapies a reality—the prime examples being artificial pancreas systems (AP systems) and Tzield.
The work of Breakthrough T1D’s Research, Advocacy, and Medical Affairs teams—in partnership with the organization’s venture philanthropy fund, the T1D Fund—will be integral to Project ACT’s success.
Like AP systems, Tzield, and all other FDA-approved drugs, treatments, and medical devices on the market today, islet cell therapies will only become available after meeting all the required benchmarks—including clinical trials.
Clinicians who are in-the-know about clinical trials and how to help their patients enroll are but one of the numerous ways Breakthrough T1D’s Project ACT will make islet cell therapies a reality, faster.
“Clinicians are generally the most trusted source for this information, but most are not making those referrals, so the gap never closes,” said Lally. “We aim to change that.”
“We want every member of the diverse T1D community to be aware of clinical trials, how to participate, and where to find information,” added Albanese-O’Neill. “The next generation of breakthroughs depends on it.”
Editor’s note: This story co-written by Ginger Vieira, special contributor to Breakthrough T1D.
While we look back on 2024, we can reflect upon the incredible progress we’ve made in advancing breakthroughs toward cures and improving everyday life with T1D.
This wouldn’t have been possible without each and every one of you and your continued support of our mission as we drive toward cures for T1D.
Here are the top 11 advances that together, we made happen in 2024:
Breakthrough T1D announced the launch of Project ACT, an initiative aimed at accelerating breakthroughs in T1D cell replacement therapies that do not require broad immunosuppression. Recent advances, such as Vertex’s stem cell-derived islets, have been made possible by Breakthrough T1D’s Cell Therapies program as part of our drive toward cures. The goal of Project ACT is to push research, development, regulatory policies, access, and adoption to increase the rate at which cell therapies without the need for broad immunosuppressants will become available to people with T1D.
Why this matters: Immunosuppressive drugs are a barrier to access to cell replacement therapies because of their toxic side effects, which is why islet transplants are currently only available to people with severe low blood sugar (hypoglycemic) unawareness and episodes. By striving toward a future where we realize the benefits of cell replacement therapies without the downsides of the current regimen of immunosuppressants, we will make islet replacement therapies broadly accessible to the T1D community.
Vertex’s clinical trial of VX-880, a first-generation stem cell-derived islet replacement therapy for people with severe hypoglycemia (requiring the use of immunosuppressants), has transitioned into a phase 1/2/3, or pivotal, trial. This news comes after Vertex shared incredibly promising data in the earlier phases of the trial, including 11 of 12 participants reducing or eliminating the need for external insulin.
The upcoming trial will expand to 50 people who will get a single, target dose of VX-880. The primary endpoint will be insulin therapy independence without severe hypoglycemic events after one year. This is the final clinical testing stage before Vertex can seek FDA approval.
Breakthrough T1D has a decades-long relationship with Vertex and the leading scientists behind stem cell-derived islet therapies, an advancement that would not have been possible without Breakthrough T1D funding and support. The T1D Fund had invested in Semma Therapeutics, which was acquired by Vertex Pharmaceuticals in 2019, eventually leading to the active clinical development of VX-880 in T1D.
Why this matters: This is the first time a scalable cure for T1D is entering phase 3 clinical trials—a significant win and a huge step toward accelerating the delivery of cell therapies to members of the T1D community!
Tegoprubart: Transplant Survival Without Standard Immunosuppressive Drugs
Tegoprubart, an anti-CD40L immunotherapy that limits the immune response, is being tested in a Breakthrough T1D-funded study in people with T1D and severe hypoglycemia who have received deceased donor islets. Eledon Pharmaceuticals announced promising initial results in which two of three people achieved insulin therapy independence. According to the study, tegoprubart is safer for both people and transplanted cells in comparison to broad immunosuppressants, with milder side effects and greater islet survival. To further support this effort, the T1D Fund: A Breakthrough T1D Venture invested in Eledon.
Cell Pouch: A Home for Transplanted Islets
Breakthrough T1D has been supporting the development of Cell Pouch, an implantable device from Sernova that provides a safe, immune-protected environment for transplanted islet cells. In phase 1/2 clinical trials, all six people who received donor islets within the Cell Pouch achieved sustained insulin therapy independence with immunosuppressants, including long-term islet survival and function over five years without harmful side effects.
Why this matters: Standard of care immunosuppressive drugs that help avoid transplant rejection come with unwelcome side effects, such as increased risk of infection and malignancy and toxicity to kidneys, nerves, and islet cells themselves. Breakthrough T1D is focused on finding alternative ways to keep transplanted islet cells alive and healthy so that cell replacement therapies can become more tolerable and accessible.
In a major effort spearheaded by Breakthrough T1D, the first internationally recognized clinical guidelines for those who test positive for T1D autoantibodies have been published. These include guidance on monitoring frequency, education, and psychosocial support in addition to recommended actions for healthcare professionals (HCPs) when the risk of T1D progression is high. The guidelines were cooperatively developed with over 60 international experts spanning ten countries.
Why this matters: Previously, there had been no consensus on monitoring guidelines for people who test positive for T1D autoantibodies. Standardization of clinical recommendations means that individuals, families, and HCPs have tangible next steps to monitor early T1D progression and catch life-threatening complications sooner.
- Breakthrough T1D is leading a campaign to secure a recommendation for T1D screening from the U.S. Preventative Services Task Force (USPSTF), the main authority for preventative care. Approval would require T1D screening to be covered by insurance—an important step forward in expanding access.
- Driven by Breakthrough T1D’s advocacy efforts, The Centers for Medicare and Medicaid Services (CMS) established a unique ICD-10 code for stage 2 T1D. ICD-10 codes are used by HCPs to classify and document diagnoses, symptoms, and procedures. These codes provide a unified way for doctors and providers to indicate what diseases or conditions a person has in their electronic health record (EHR), empowering HCPs to document accurate diagnoses and provide the best possible care.
Why this matters: T1D early detection is critically important to prevent life-threatening complications at diagnosis and to give people necessary resources to make informed decisions about their health. Integrating T1D screening into the U.S. healthcare system will increase access to care.
The past year has seen some important advances in glucose management therapies and devices:
- Cadisegliatin, an activator of a blood sugar regulator in the liver, is being investigated in a phase 3 clinical trial (TTP399) as an adjunct therapy to insulin for people with T1D, although it is currently placed on clinical hold. vTv Therapeutics, the trial sponsor, is also a T1D portfolio company.
- The Omnipod 5 app is now available for the iPhone, making it easier to control the Omnipod without the need to carry a controller. It can also integrate with the Dexcom G6 continuous glucose monitor (CGM).
- Eversense 365 is the first FDA-approved year-round sensor that can easily integrate with automated insulin delivery (AID) systems. Other sensors require replacement after 10-14 days.
Why this matters: While advancements in glucose management have been pivotal in improving health outcomes for people with T1D, access remains a challenge. AID systems are globally underutilized, and not everyone has the necessary technology to connect devices. Breakthrough T1D is working to not only support advances in glucose management but also increase access.
Related content: While Breakthrough T1D consistently strives to improve the lives of those living with T1D, as an organization we have made incredible progress in the development of AID systems, also called the artificial pancreas systems. Read a historical perspective written by Breakthrough T1D volunteer Doug Lowenstein that covers conception to FDA approval of the first artificial pancreas systems, which changed the lives of people with T1D.
An inquiry spearheaded by the Breakthrough T1D affiliates in the U.K. uncovered risks of developing T1D eating disorders (T1DE), including bulimia, anorexia, or insulin restriction to lose weight. There is a significant gap in education and clinical guidelines for HCPs, a lack of internationally recognized criteria for T1DE diagnosis, and insufficient care integration, leading to preventable complications and healthy years of life lost. Breakthrough T1D recognizes the importance of spreading awareness and support for T1DE, and much work is needed to improve the lives of those living with T1DE.
Why this matters: There is an urgent need to change the way T1DE is approached, including integrated physical care with mental health services to get people with T1DE the access to care that they need.
In a study that included people with T1D, finerenone (Kerendia®) has been shown to improve cardiovascular outcomes in adults with heart failure. The drug is already approved in the U.S. to treat kidney and cardiovascular disease in people with T2D. Based on these results, Breakthrough T1D is supporting a clinical trial (FINE-ONE) in conjunction with Bayer to investigate the use of finerenone for T1D with the hopes of reducing kidney complications.
Why this matters: Kidney and cardiovascular disease remain significant challenges for those with T1D, especially given the FDA’s recent rejection of an SGLT inhibitor to lower blood glucose in people with T1D and chronic kidney disease. Yet, a new clinical trial (SUGARNSALT) will better assess the benefits versus risks.
Breakthrough T1D is advocating for the regulatory approval of C-peptide, a biomarker for insulin production by beta cells, to be used as an endpoint in clinical trials. An endpoint can accurately predict a meaningful benefit in clinical trials for disease-modifying therapies (DMTs; treatments that can slow, halt, or reverse T1D). To support this endeavor, Breakthrough T1D scientists and an expert consensus panel published research with evidence supporting C-peptide as an endpoint. Breakthrough T1D is continuing to engage with regulators, coordinate with industry, and assess more clinical trial data to drive this effort forward.
Why this matters: Current clinical trial endpoints (HbA1c, hypoglycemia, and complications) are not the best way to gauge the clinical benefits of T1D therapies. If C-peptide gets regulatory approval to be used as an endpoint, clinical trials could be smaller and shorter while still accurately assessing the advantages of a DMT. This means that drug development can move more quickly, and people with T1D will be able to access therapies sooner.
Related content: Two years ago, the T1D community received the incredible news that Tzield® had become the first FDA-approved disease-modifying therapy that can significantly delay T1D onset. Breakthrough T1D volunteer Doug Lowenstein recounts the life-changing drug’s journey nearly 100 years after the discovery of insulin.
The T1D Index is a data simulation tool that measures the global health impact of T1D, bridging gaps in our knowledge of public health statistics. T1D Index 2.0 has new and improved functionality, including advanced simulation capabilities, validation of data, and enhanced user experience. Breakthrough T1D contributed to both the development and improvement of the T1D Index.
Why this matters: The T1D index is critical in defining the intercontinental scope of T1D, driving us toward country-specific solutions and improved global health outcomes.
Earlier this year, JDRF rebranded to Breakthrough T1D. While our mission remains the same, our name needs to better reflect who we are and where we’re going. Our new brand aligns with our mission to accelerate life-changing breakthroughs for those of every age living with T1D as we work toward a world without it.
Why this matters: The proof is in the name—each day we strive to increase and accelerate breakthroughs in T1D, and it’s critical for our brand to accurately reflect our mission.
It’s certainly been an exciting year! While we still have more work to do, it’s crucial to celebrate our wins, both big and small, to see how far we’ve come in our push to make T1D a thing of the past.
Together, we’re accelerating breakthroughs for people with T1D, and the support of the T1D community drives our mission forward every single day, leading the way to lifechanging therapies and cures. Let’s see what 2025 has in store!
It’s early October, which means the Nobel Prizes are being awarded in several categories. These prestigious awards recognize outstanding contributions in Peace, Literature, Physics, Chemistry, Physiology or Medicine, and Economic Sciences. They go to the best and brightest people with the best and brightest ideas.
This year, the prizes recognize work that is, in several ways, connected to Breakthrough T1D and the work we are doing to cure type 1 diabetes (T1D) and improve the lives of those living with it.
microRNAs
The 2024 Nobel Prize in Physiology or Medicine was awarded to Victor Ambros and Gary Ruvkun for the discovery of microRNA and its role in post-transcriptional gene regulation.
But what is it?
The DNA in our body has between 20,000 and 25,000 genes. Our body constantly activates those genes, which allows it to function. For example, there is a gene that tells the beta cells to start creating insulin in response to elevated blood glucose levels.
This is called gene expression—it’s when the body produces something, usually a protein, to do something specific in the body. Gene expression happens when the DNA of a gene is copied to form messenger RNA, or mRNA, which is then turned into a protein that has a unique function. This is orchestrated in a highly tissue-specific manner, creating diverse cell types like muscle, nerve, beta cell, and more.
In 1993, we learned that molecules called microRNAs regulate gene expression. They can hamper or promote it. By measuring the presence of microRNAs and using them as a biomarker, we can learn a lot about what is going on inside the body, what genes are being expressed, and in which cell types.
How does this apply to type 1 diabetes?
Breakthrough T1D is actively funding research into the use of microRNAs to advance our mission. In fact, we are currently funding $2.6 million in grants related to microRNAs. Specifically, we’re exploring their use as biomarkers of disease progression and as a therapeutic target to interfere with the autoimmunity behind T1D.
Biomarkers
Biomarkers are, put very simply, things in the body that can be measured. Pulse, body temperature, and blood pressure are all biomarkers. In T1D, there are a handful used in common parlance: blood glucose level, HbA1c, time-in-range, autoantibody status, and more. We want to validate the use of microRNAs as a biomarker of disease progression.
We know through years of work that early detection has many benefits. This includes being educated on what T1D is, preparing for a potential diagnosis, the ability to benefit from a disease-modifying therapy to delay onset, and preventing potentially life-threatening complications at onset. microRNAs have the potential to increase our understanding of disease progression and identify how quickly a person is progressing.
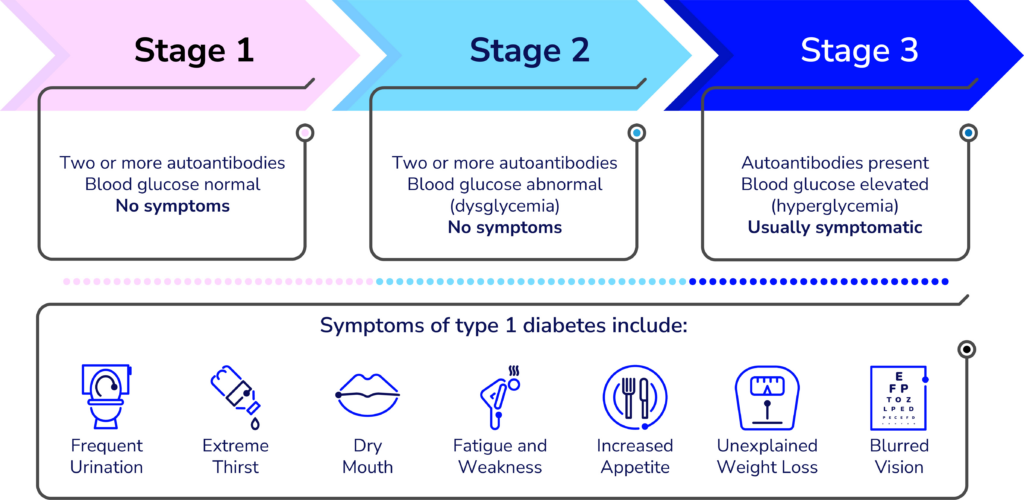
Type 1 diabetes occurs in stages. Today, biomarkers of progression, like autoantibody status, don’t paint the whole picture. If a person tests positive for 2 autoantibodies, that means they are almost 100% likely to develop T1D at some point—but we don’t know how fast. We can measure blood glucose levels, but that is a single data point for dysglycemia. It doesn’t tell us how healthy the beta cells are.
microRNAs have the potential to paint a much more detailed picture. We are funding research to discover whether we can use microRNAs to learn exactly where a person is in their progression to stage 3 T1D and how quickly it’s happening.
In summary—we believe microRNAs can enhance the predictive value on top of the current biomarkers for T1D. They can be a very useful tool in measuring progression and helping people in stages 1 and 2 of T1D.
microRNAs as a therapeutic target
Type 1 diabetes is an autoimmune disease—a disease where the body’s immune system destroys its own cells. In T1D, the T-cells in the immune system destroy the insulin-producing cells in the pancreas.
Our research into stopping disease progression focuses mainly on two areas: modifying the immune system and modifying the beta cells. microRNAs can potentially help us fix the dysregulation in the immune system, slowing down or halting the autoimmune attack.
Breakthrough T1D-funded researchers discovered that blocking microRNA-146a in mice can prevent the T-cells from damaging the beta cells. Preventing damage to the beta cells prevents T1D from progressing. Our hypothesis: if we can block microRNA-146a, we can slow down or halt disease progression. This specific study is in a pre-clinical setting, and if it goes well, it could move into clinical trials in the near future.
David Baker – Nobel Prize in Chemistry
David Baker, a breakthrough T1D-funded researcher, was awarded half the 2024 Nobel Prize in Chemistry for computational protein design.
Baker’s prize acknowledges his work in discovering a way to create new proteins that have never existed before. These proteins can potentially be used to treat diseases, make new vaccines, and more. A few years ago, we saw a potential application to T1D.
There haven’t been any groundbreaking changes in insulin since the discovery of synthetic insulin in the late 1970’s. Breakthrough T1D wants to change that—and is funding researchers, like David Baker, to figure out what the next generation of insulins can look like.
Baker received two grants from us from 2016-2021 to use a computer model to create new, glucose-responsive insulin (GRI). GRI is insulin that can be administered, exist in the blood stream, and only be active when it is needed. Baker’s grant was one of many projects we are pursuing in GRI. This work continues to this day, and there are even GRIs in human clinical trials.
What’s next?
This year’s Nobel Prizes show that we are focusing on the same things the Nobel Committee is focused on: the best and brightest scientists and the best and brightest research. Hopefully, one day, we’ll see a T1D scientist win a Nobel Prize for curing this disease.
Want to learn more?
Visit our Funded Research page, where you can read about every single grant we fund—including David Baker’s work in GRI and the many grants currently being funded to study microRNAs.
On October 1st, the T1D community got a big win: the Centers for Medicare and Medicaid Servies (CMS) introduced a unique ICD-10 code for stage 2 type 1 diabetes (T1D). This addresses a significant gap in clinical care. Prior to this change, clinicians had limited options for coding stage 2 T1D, which resulted in inaccurate patient records.
This may seem like a minor detail but it’s critical! It will profoundly affect physicians’ abilities to diagnose and treat people with stage 2 T1D.
What is an ICD-10 Code?
ICD-10 codes are codes used by healthcare providers to classify and document diagnoses, symptoms, and procedures. These codes provide a unified way for doctors and providers to indicate what diseases or conditions a person has in their electronic health record (EHR).
The ICD-10 code for stage 3 T1D, or clinical diagnosis of T1D is E10. If that code is in a person’s EHR, a physician immediately knows that they have T1D. Having that information can help them provide proper care to their patients.
What Is Stage 2 T1D?
Stage 2 T1D is defined by the presence of autoimmune antibodies (AAB). Autoantibodies are proteins in the blood that indicate the body’s immune system is attacking the insulin-producing cells in the pancreas. People in stage 2 are usually asymptomatic, but they can experience dysglycemia, or abnormal blood sugar levels.
The only way individuals can find out if they are in stage 2 T1D is through antibody screening.
Why does this matter?
Stage 2 and stage 3 T1D are not the same. They are not managed in the same way or treated in the same way. For a healthcare provider to give the appropriate care, they need the correct diagnosis.
The previous lack of an ICD-10 code for this early stage of T1D meant that individuals could be misclassified, either reflecting stage 3 T1D or no T1D at all. This means they may not be getting the proper care and monitoring of the disease’s potential progression.
Here’s how this changes T1D management:
The introduction of a specific code for stage 2 T1D has significant implications.
Enhanced monitoring and education
- Recognizing individuals in stage 2 allows healthcare providers to deliver the right education on monitoring so they can prepare for stage 3. This can eliminate diabetic ketoacidosis, a life-threatening condition that can occur at diagnosis.
Access to new therapies
- Individuals diagnosed in stage 2 may be eligible for an FDA-approved disease-modifying therapy that delays onset of stage 3 for an average of two years.
Research opportunities
- Many recruiting clinical trials are available for people with stage 2 and 3 T1D. If individuals are coded correctly, they can better take advantage of these studies and play a crucial role in developing the next generation of T1D therapies.
Evidence-based care
- Accurate coding ensures that healthcare providers can deliver evidence-based clinical care. If a diagnosis is not documented correctly, it may result in missed opportunities for intervention and support.
How this happened
Breakthrough T1D played a significant role in advocating for the creation and adoption of this code. We crafted a letter in support of this code that several of our peer organizations signed onto. We also galvanized the clinical side to add their support to this initiative, all of which were instrumental in the code creation and adoption.
A big step forward
The recent introduction of ICD-10 codes for Stage 2 T1D is a significant step forward for the T1D community. By accurately identifying individuals at this critical stage of T1D, healthcare providers can treat and monitor them accordingly, improving both patient outcomes and enhancing our understanding and management of T1D.