Type 1 diabetes (T1D) is caused by the autoimmune destruction of insulin-producing beta cells in the pancreas. People with T1D are dependent on insulin therapy to control their blood sugar levels, which is critical to prevent complications that occur when blood sugar is too high (hyperglycemia) or too low (hypoglycemia).
The best bet for T1D cures depends on cell therapies, which replace destroyed beta cells with protected, functional cells to restore insulin therapy independence and glucose control, ideally without chronic immunosuppression. Breakthrough T1D’s Cures Program has been instrumental in the incredible progress we’ve made in cell therapies research. The secret to success? Stem cells.
What are stem cells?
Stem cells are uniquely suited for use in cell therapies because of their biological characteristics. First, they are essentially a blank slate—we can biologically engineer them to become any cell we want, including beta cells. Second, stem cells can make copies of themselves while remaining a blank slate, meaning we can generate an unlimited source of transformable cells.
Since scientists first isolated human stem cells in 1998, there has been major progress in therapies that can replace or renew damaged and diseased tissue. For example, people with blood cancer often undergo chemotherapy and radiation to destroy cancerous blood cells. Stem cells are delivered directly into the bloodstream and travel to the bone marrow, where they transform into new, non-cancerous blood cells, replacing the important cells that were lost with healthy ones. The exciting progress in stem cell research extends to T1D—researchers have harnessed the power of stem cells to generate functional beta cells and islets, rapidly accelerating the drive toward T1D cures. Breakthrough T1D has been at the forefront of stem cell research in T1D for decades.
Stem cells are the foundation of our Cell Therapies Program
Breakthrough T1D’s Cell Therapies Program focuses solely on making and improving stem cell-derived beta cells. For stem cell-based therapies to become a reality for everyone with T1D, there are three primary goals that we are striving to achieve:
- First, we need to generate a renewable, scalable source of beta cells so that there are enough for everyone who needs them.
- Second, we need to find a habitable site to implant beta cells so that they remain functional and healthy for very long periods of time.
- Third, we must find a way to protect implanted beta cells from immune attack so that people won’t need to take chronic anti-rejection immunosuppressants, which can come with intolerable side effects.
Breakthrough T1D has put tremendous effort into achieving these goals; we’ve seen incredible progress in recent years, pushing us closer than ever to cures for T1D.
Breakthrough T1D has driven more than $156 million to cell therapies research in the past decade and has spearheaded several initiatives to drive this effort forward. In 2013, the Beta Cell Replacement Consortium was launched, bringing together 50+ of the brightest scientists and key industry players to integrate expertise in bioengineering, animal models, transplant medicine, and other key research areas.
Similarly, Breakthrough T1D established several Centers of Excellence, a collection of institutions driving exceptional advancements in immunology, stem cell biology, and gene editing, all of which are critically important to cell therapies research. The ultimate goal of these initiatives is to foster collaboration, exchange resources and data, and accelerate the development of stem cell-derived islet therapies.
Project ACT
To further support these efforts, Breakthrough T1D most recently launched Project Accelerate Cell Therapies (Project ACT) to simultaneously push research, development, regulatory policies, access, and adoption to increase the rate at which cell therapies without the need for broad immunosuppression will become available to people with T1D. This is important because, at this time, cell therapies require anti-rejection immunosuppressants, which can come with serious long-term side effects that may not be tolerable for everyone with T1D.
Looking forward
With Breakthrough T1D’s commitment to driving cell therapies forward, we have made significant headway in the development of life-changing therapies that can place healthy, insulin-producing beta cells back into people with T1D. “Even with today’s fantastic automated insulin delivery systems and advanced algorithms, those living with T1D still spend a significant amount of time interacting with their devices in order to maintain blood sugar control,” said Nicholas Mamrak, a scientist at Breakthrough T1D. “The prospect of cell therapies lies in the ability to take off these pumps and spend less time managing and worrying about their diabetes.”
The drive toward stem cell-based therapies becoming a reality for everyone with T1D continues—despite how far we’ve come, we still have more work to do.
This article is the first of a series exploring the different ways that Breakthrough T1D’s Project ACT (Accelerate Cell Therapies) will shape the future of cell therapies for type 1 diabetes (T1D). Stay tuned for the next article, which will explore the present and future of cell therapies for T1D.
Today, Sana Biotechnology released significant clinical data: the first person with type 1 diabetes (T1D) who received deceased donor islets engineered to evade the immune system is producing insulin without immunosuppression.
The details
This is a big step for cell-based therapies for T1D. Sana’s first-in-human study consists of allogeneic islets, meaning they are derived from an external source, which in this case is the pancreases of deceased donors. These islets were engineered to avoid recognition by the immune system (hypoimmune) and were implanted intramuscularly into a person with T1D. After four weeks, circulating C-peptide increased, meaning that the beta cells are alive, healthy, and producing insulin—all without the need for immunosuppression and no safety issue. This is the first evidence of engineered islets successfully avoiding immune destruction.
What this means for the T1D community
While this is an incredibly promising step forward for the T1D community, currently available cell therapies that rely on deceased donor islets (Lantidra®) are only accessible to a small portion of the T1D population because there are very few donor cells available. They also require broad anti-rejection immunosuppressants, which can come with serious side effects that may not be manageable for everyone with T1D. Engineering cells to evade immune attack is a new path forward to protect the insulin-producing beta cells and avoid the use of immunosuppressants. Most importantly, this technology can now be applied to stem cell-based therapies, which is a scalable solution for many people with T1D.
What’s next: lots to look forward to
Breakthrough T1D believes that the best bet for type 1 diabetes cures lies in stem cell-based therapies since deceased donor islets are in short supply, while stem cell-derived islets can be produced at scale. We have now opened the doors to apply hypoimmune technology to stem cell-derived islets, moving us closer to the possibility of having enough immune-evading cells for everyone with T1D. While this will take significant time, effort, and money, every day we take another step toward a possible life-changing T1D cure.
Breakthrough T1D’s role
The primary objective of Breakthrough T1D’s beta cell replacement efforts is to place insulin-producing cells into people with T1D without the use of immunosuppressants. Breakthrough T1D strongly supports the development of stem cell-based therapies that do not require broad immunosuppression and recently launched an initiative to accelerate this faster than ever (Project ACT – Accelerate Cell Therapies). To contribute to the advancement of these game-changing therapies, the T1D Fund: A Breakthrough T1D Venture invested in Sana recognizing that their hypoimmune engineering technology held significant promise for type 1 diabetes cell therapies. We look forward to seeing how the trial progresses.
While we look back on 2024, we can reflect upon the incredible progress we’ve made in advancing breakthroughs toward cures and improving everyday life with T1D.
This wouldn’t have been possible without each and every one of you and your continued support of our mission as we drive toward cures for T1D.
Here are the top 11 advances that together, we made happen in 2024:
Breakthrough T1D announced the launch of Project ACT, an initiative aimed at accelerating breakthroughs in T1D cell replacement therapies that do not require broad immunosuppression. Recent advances, such as Vertex’s stem cell-derived islets, have been made possible by Breakthrough T1D’s Cell Therapies program as part of our drive toward cures. The goal of Project ACT is to push research, development, regulatory policies, access, and adoption to increase the rate at which cell therapies without the need for broad immunosuppressants will become available to people with T1D.
Why this matters: Immunosuppressive drugs are a barrier to access to cell replacement therapies because of their toxic side effects, which is why islet transplants are currently only available to people with severe low blood sugar (hypoglycemic) unawareness and episodes. By striving toward a future where we realize the benefits of cell replacement therapies without the downsides of the current regimen of immunosuppressants, we will make islet replacement therapies broadly accessible to the T1D community.
Vertex’s clinical trial of VX-880, a first-generation stem cell-derived islet replacement therapy for people with severe hypoglycemia (requiring the use of immunosuppressants), has transitioned into a phase 1/2/3, or pivotal, trial. This news comes after Vertex shared incredibly promising data in the earlier phases of the trial, including 11 of 12 participants reducing or eliminating the need for external insulin.
The upcoming trial will expand to 50 people who will get a single, target dose of VX-880. The primary endpoint will be insulin therapy independence without severe hypoglycemic events after one year. This is the final clinical testing stage before Vertex can seek FDA approval.
Breakthrough T1D has a decades-long relationship with Vertex and the leading scientists behind stem cell-derived islet therapies, an advancement that would not have been possible without Breakthrough T1D funding and support. The T1D Fund had invested in Semma Therapeutics, which was acquired by Vertex Pharmaceuticals in 2019, eventually leading to the active clinical development of VX-880 in T1D.
Why this matters: This is the first time a scalable cure for T1D is entering phase 3 clinical trials—a significant win and a huge step toward accelerating the delivery of cell therapies to members of the T1D community!
Tegoprubart: Transplant Survival Without Standard Immunosuppressive Drugs
Tegoprubart, an anti-CD40L immunotherapy that limits the immune response, is being tested in a Breakthrough T1D-funded study in people with T1D and severe hypoglycemia who have received deceased donor islets. Eledon Pharmaceuticals announced promising initial results in which two of three people achieved insulin therapy independence. According to the study, tegoprubart is safer for both people and transplanted cells in comparison to broad immunosuppressants, with milder side effects and greater islet survival. To further support this effort, the T1D Fund: A Breakthrough T1D Venture invested in Eledon.
Cell Pouch: A Home for Transplanted Islets
Breakthrough T1D has been supporting the development of Cell Pouch, an implantable device from Sernova that provides a safe, immune-protected environment for transplanted islet cells. In phase 1/2 clinical trials, all six people who received donor islets within the Cell Pouch achieved sustained insulin therapy independence with immunosuppressants, including long-term islet survival and function over five years without harmful side effects.
Why this matters: Standard of care immunosuppressive drugs that help avoid transplant rejection come with unwelcome side effects, such as increased risk of infection and malignancy and toxicity to kidneys, nerves, and islet cells themselves. Breakthrough T1D is focused on finding alternative ways to keep transplanted islet cells alive and healthy so that cell replacement therapies can become more tolerable and accessible.
In a major effort spearheaded by Breakthrough T1D, the first internationally recognized clinical guidelines for those who test positive for T1D autoantibodies have been published. These include guidance on monitoring frequency, education, and psychosocial support in addition to recommended actions for healthcare professionals (HCPs) when the risk of T1D progression is high. The guidelines were cooperatively developed with over 60 international experts spanning ten countries.
Why this matters: Previously, there had been no consensus on monitoring guidelines for people who test positive for T1D autoantibodies. Standardization of clinical recommendations means that individuals, families, and HCPs have tangible next steps to monitor early T1D progression and catch life-threatening complications sooner.
- Breakthrough T1D is leading a campaign to secure a recommendation for T1D screening from the U.S. Preventative Services Task Force (USPSTF), the main authority for preventative care. Approval would require T1D screening to be covered by insurance—an important step forward in expanding access.
- Driven by Breakthrough T1D’s advocacy efforts, The Centers for Medicare and Medicaid Services (CMS) established a unique ICD-10 code for stage 2 T1D. ICD-10 codes are used by HCPs to classify and document diagnoses, symptoms, and procedures. These codes provide a unified way for doctors and providers to indicate what diseases or conditions a person has in their electronic health record (EHR), empowering HCPs to document accurate diagnoses and provide the best possible care.
Why this matters: T1D early detection is critically important to prevent life-threatening complications at diagnosis and to give people necessary resources to make informed decisions about their health. Integrating T1D screening into the U.S. healthcare system will increase access to care.
The past year has seen some important advances in glucose management therapies and devices:
- Cadisegliatin, an activator of a blood sugar regulator in the liver, is being investigated in a phase 3 clinical trial (TTP399) as an adjunct therapy to insulin for people with T1D, although it is currently placed on clinical hold. vTv Therapeutics, the trial sponsor, is also a T1D portfolio company.
- The Omnipod 5 app is now available for the iPhone, making it easier to control the Omnipod without the need to carry a controller. It can also integrate with the Dexcom G6 continuous glucose monitor (CGM).
- Eversense 365 is the first FDA-approved year-round sensor that can easily integrate with automated insulin delivery (AID) systems. Other sensors require replacement after 10-14 days.
Why this matters: While advancements in glucose management have been pivotal in improving health outcomes for people with T1D, access remains a challenge. AID systems are globally underutilized, and not everyone has the necessary technology to connect devices. Breakthrough T1D is working to not only support advances in glucose management but also increase access.
Related content: While Breakthrough T1D consistently strives to improve the lives of those living with T1D, as an organization we have made incredible progress in the development of AID systems, also called the artificial pancreas systems. Read a historical perspective written by Breakthrough T1D volunteer Doug Lowenstein that covers conception to FDA approval of the first artificial pancreas systems, which changed the lives of people with T1D.
An inquiry spearheaded by the Breakthrough T1D affiliates in the U.K. uncovered risks of developing T1D eating disorders (T1DE), including bulimia, anorexia, or insulin restriction to lose weight. There is a significant gap in education and clinical guidelines for HCPs, a lack of internationally recognized criteria for T1DE diagnosis, and insufficient care integration, leading to preventable complications and healthy years of life lost. Breakthrough T1D recognizes the importance of spreading awareness and support for T1DE, and much work is needed to improve the lives of those living with T1DE.
Why this matters: There is an urgent need to change the way T1DE is approached, including integrated physical care with mental health services to get people with T1DE the access to care that they need.
In a study that included people with T1D, finerenone (Kerendia®) has been shown to improve cardiovascular outcomes in adults with heart failure. The drug is already approved in the U.S. to treat kidney and cardiovascular disease in people with T2D. Based on these results, Breakthrough T1D is supporting a clinical trial (FINE-ONE) in conjunction with Bayer to investigate the use of finerenone for T1D with the hopes of reducing kidney complications.
Why this matters: Kidney and cardiovascular disease remain significant challenges for those with T1D, especially given the FDA’s recent rejection of an SGLT inhibitor to lower blood glucose in people with T1D and chronic kidney disease. Yet, a new clinical trial (SUGARNSALT) will better assess the benefits versus risks.
Breakthrough T1D is advocating for the regulatory approval of C-peptide, a biomarker for insulin production by beta cells, to be used as an endpoint in clinical trials. An endpoint can accurately predict a meaningful benefit in clinical trials for disease-modifying therapies (DMTs; treatments that can slow, halt, or reverse T1D). To support this endeavor, Breakthrough T1D scientists and an expert consensus panel published research with evidence supporting C-peptide as an endpoint. Breakthrough T1D is continuing to engage with regulators, coordinate with industry, and assess more clinical trial data to drive this effort forward.
Why this matters: Current clinical trial endpoints (HbA1c, hypoglycemia, and complications) are not the best way to gauge the clinical benefits of T1D therapies. If C-peptide gets regulatory approval to be used as an endpoint, clinical trials could be smaller and shorter while still accurately assessing the advantages of a DMT. This means that drug development can move more quickly, and people with T1D will be able to access therapies sooner.
Related content: Two years ago, the T1D community received the incredible news that Tzield® had become the first FDA-approved disease-modifying therapy that can significantly delay T1D onset. Breakthrough T1D volunteer Doug Lowenstein recounts the life-changing drug’s journey nearly 100 years after the discovery of insulin.
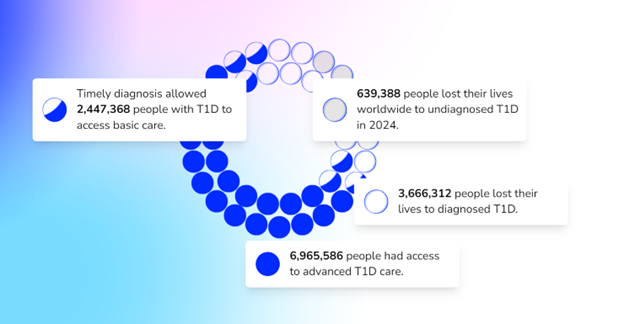
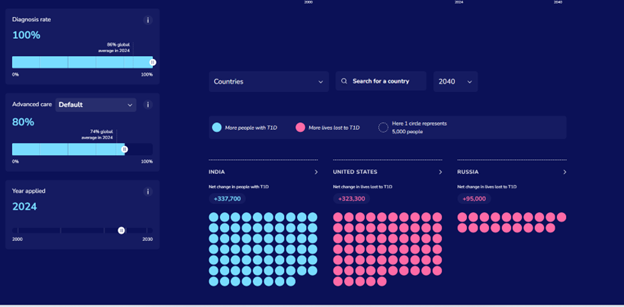
The T1D Index is a data simulation tool that measures the global health impact of T1D, bridging gaps in our knowledge of public health statistics. T1D Index 2.0 has new and improved functionality, including advanced simulation capabilities, validation of data, and enhanced user experience. Breakthrough T1D contributed to both the development and improvement of the T1D Index.
Why this matters: The T1D index is critical in defining the intercontinental scope of T1D, driving us toward country-specific solutions and improved global health outcomes.
Earlier this year, JDRF rebranded to Breakthrough T1D. While our mission remains the same, our name needs to better reflect who we are and where we’re going. Our new brand aligns with our mission to accelerate life-changing breakthroughs for those of every age living with T1D as we work toward a world without it.
Why this matters: The proof is in the name—each day we strive to increase and accelerate breakthroughs in T1D, and it’s critical for our brand to accurately reflect our mission.
It’s certainly been an exciting year! While we still have more work to do, it’s crucial to celebrate our wins, both big and small, to see how far we’ve come in our push to make T1D a thing of the past.
Together, we’re accelerating breakthroughs for people with T1D, and the support of the T1D community drives our mission forward every single day, leading the way to lifechanging therapies and cures. Let’s see what 2025 has in store!
A novel immune therapy called tegoprubart made by Eledon Pharmaceuticals and being tested in kidney transplant patients has the potential to help beta cell transplants survive in people with type 1 diabetes (T1D) with fewer side effects. The first data from this Breakthrough T1D-funded study suggests it does. The study was presented at the 5th Annual International Pancreas and Islet Transplant Association/Harvard Stem Cell Institute/Breakthrough T1D Stem Cells Summit.
The need for a better drug regimen
Organ transplants are a wonder of modern medicine, but they require the use of immunosuppressive drugs. These drugs have serious side effects. They include but are not limited to an increased risk of infections and malignancies. They are also toxic to the kidneys, nerves, and islet cells themselves.
This is one reason that islet transplants, which follow the Edmonton Protocol, are only an option for people with hypoglycemia unawareness who have had severe hypoglycemic events. (Another reason is the extremely limited supply of deceased donor islets.) Today, Breakthrough T1D and researchers across various disciplines are working on developing novel and more targeted drugs. They goal: develop drugs that can inhibit the immune response to transplanted cells, like pancreatic islets, with more tolerable, or milder, side effects.
If the more serious side effects can be prevented, a much larger population of people with T1D could have access to this therapy. That is, assuming we have a larger supply of cells to transplant.
Enter tegoprubart
Tegoprubart is an immune therapy (anti-CD40 ligand) manufactured by Eledon Pharmaceuticals. It helps limit the body’s immune response.
It works by inhibiting CD-40L, a protein involved in the immune system. By blocking this protein, the drug interferes with how immune cells communicate with each other. It also increases the number of T regulatory cells, which suppress the body’s immune response.
This drug is currently in a phase 3 clinical trial in kidney transplants conducted by Eledon Pharmaceuticals. Results to date indicate that it has the potential to be a less toxic option to keep transplanted organs and cells, like islet cells, alive and healthy post-transplant.
Early results from new study are positive—and more data is needed
Breakthrough T1D is funding longtime collaborator Dr. Piotr Witkowski at the University of Chicago to use Eledon Pharmaceutical’s drug, tegroprubart, as an alternative to traditional immunosuppressives in people with T1D and severe hypoglycemia who have received deceased donor islet transplants.
Per Eledon Pharmaceutical’s press release:
- The first two out of three subjects treated with tegoprubart as part of an immunosuppression regimen to prevent transplant rejection achieved insulin independence. They remained insulin-free, with glucose control in the normal range.
- The third subject was recently transplanted. They reduced insulin dosage by 60% within three days post-transplant.
- Islet engraftment in the first two subjects with tegoprubart was three to five times higher than engraftment in three subjects receiving standard-of-care tacrolimus-based immunosuppression.
- Treatment with tegoprubart was well tolerated.
This news is exciting and has the potential to be life-changing for people with T1D. Removing the 24/7, 365-day-a-year burden of T1D without toxic side effects through curative therapies is our goal.
However, the data is only in two people to date. We look forward to seeing data from more transplants in the future.
How this fits into our strategy for cures
Breakthrough T1D is laser-focused on cell therapies, which implant insulin-producing cells into the bodies of people with T1D. Our ultimate goal is an unlimited, or allogenic, supply of cells derived from stem cells. These cells can be transplanted into anyone living with T1D without the use of chronic immunosuppressives.
In other words, we need two things: a unlimited cell source and a non-toxic way to keep the cells healthy.
Incredible recent progress has been made toward both of these goals. For example, in Vertex’s VX-880 study, they are using stem-cell-derived islets, and the 11/12 recipients are fully insulin-independent after 1 year. Individuals in this study are on the traditional post-transplant immunosuppressive regimen. (The study is ongoing and has expanded enrollment to 37 people.)
Breakthrough T1D, Vertex, and others are also working on how to keep the cells safe using a combination of encapsulation, gene editing, and other tactics. Several of these studies are in clinical trials.
Tegoprubart can potentially be a viable tactic to keep these cells functional durably. That’s why we’re funding the study along with the Cure Alliance. It’s also why the T1D Fund invested in Eledon Pharmaceuticals several months ago and again on October 29.
What we’re saying
“Breakthrough T1D is proud to fund and support this research and is encouraged by the tegoprubart study showing that patients who received islet transplants with a tacrolimus-free immunosuppressive regimen are making insulin again,” said Breakthrough T1D Chief Scientific Officer Sanjoy Dutta, Ph.D. “Islet replacement therapies are a key priority for Breakthrough T1D, and we’re committed to driving research that moves us toward a world where these therapies are available to the broader T1D community. Achieving this requires novel approaches to keep transplanted cells functional with a tolerable immunosuppression regimen. These results are an important step toward that goal, and we look forward to seeing additional data.”
Read more in the press release.
At the 2024 International Society for Pediatric and Adolescent Diabetes (ISPAD) Conference in Lisbon, Portugal, the world’s leading diabetes researchers, academics, and members of industry gathered to share the latest and greatest in diabetes research. Breakthrough T1D leaders and many of our funded researchers and collaborators were on hand —for ISPAD’s 50th birthday—to share new science, breakthroughs, and a glimpse at what the next generation of T1D therapies will look like.
Let’s look at a few highlights!
The T1D Index Levels Up

Breakthrough T1D Chief Scientific Officer Sanjoy Dutta, Ph.D., and Thomas Danne, MD, Chief Medical Officer, International presented a much-awaited update on the T1D Index at ISPAD.
The T1D Index is a first-of-its-kind data simulation tool that measures the human and public health impact of the T1D crisis in every country across the globe. Until the creation of the Index, there have been wide gaps in the data about the incidence and impact of T1D. Leveraging data and insights from the T1D Index can help change the lives of people living with T1D by identifying attainable country-by-country interventions, including timely diagnosis, accessible care, and funding research that could lead to cures.
First , Dr. Dutta gave a refresher on our recent brand evolution, which includes why this change was necessary and how our research strategy has not changed.
Dr. Danne followed with a reintroduction of the Index, its place in our mission, and how we improved it. This includes:
- An enhanced dashboard and user interface designed to improve user experience
- A plan to develop Index 2.0
- An invitation and plea for all countries and existing registries to collaborate with data to enhance and develop Index 2.0
- Advanced simulation capabilities allowing for scenario analysis.
- Validation of data against available national registry data.
- Performance upgrades, including improved platform speed and minor adjustments to further refine accuracy.
In the future, the Index aims to have even more detailed data on a regional level.
Key takeaway:
Breakthrough T1D is focused on improving the lives of people with T1D all around the world—that includes every country in the world. The Index is key to defining the global scope of T1D and the country-by-country solutions to bring better outcomes to everyone affected by T1D.
Is metabolic control enough for young people with T1D?
We have known for decades that T1D is accompanied by the risk of developing complications. The conditions that are most associated with T1D include diabetic eye disease (retinopathy), kidney disease (nephropathy), and heart disease (cardiovascular disease). This is not an exhaustive list—there are many others, including mental health disorders. These complications most commonly occur in adults living with T1D, but new research suggests there’s more we can do to monitor and intervene with these complications in youths with T1D in addition to striving for ideal glycemic control.
At ISPAD, Breakthrough T1D-funded researcher Risa Wolf, MD, discussed long-term microvascular and macrovascular complications in T1D, including the complications mentioned above, and the data is striking. There is a low percentage of complications 4-7 years after diagnosis but after 12 years:
- 24% will have a decline in eGFR (a biomarker for kidney function)
- 13% will have neuropathy
- 52% will have retinopathy
- 28% will have dyslipidemia (abnormal levels of lipids in the blood)
Thankfully, leaps in care management, including automated insulin delivery systems and continuous glucose monitors, have led to improvements in A1c and, in turn, the rate at which people develop complications. But more can be done.
Through regular screening for these more common complications for all youths with T1D, we can better identify, diagnose, and monitor individuals as they develop these complications—especially because many of these screenings are low-cost.
Breakthrough T1D, for example, is funding Dr. Wolf to use the autonomous AI system (IDx-DR, Digital Diagnostics), which is FDA-approved for adults 21+ to detect and diagnose diabetic retinopathy in children. Ideally, this will lead to FDA approval and a better tool for monitoring this complication in kids.
Drs. M. Loredana Marcovecchio – another Breakthrough T1D funded investigator and Didac Mauricio took a similar look at vascular complications. Their presentations had related themes—it is critical to develop ways to identify complications like cardiovascular disease earlier. If they’re identified earlier, individuals can take advantage of the approved therapies.
Key Takeaway:
Like most areas of T1D management: there are still significant unmet needs.
We need to have a long view of these complications and their pathogenesis, which can start in youth. Glycemic control is critical to preventing the onset of these complications, but it is not always enough. Cardiovascular disease, retinopathy, dyslipidemia, and more can all be detected at a young age, which gives more time for interventions.
Breakthrough T1D is working on all of this in our Improving Lives program.
ISPAD / Breakthrough T1D Sessions
Breakthrough T1D Chief Scientific Officer Sanjoy Dutta, Ph.D. joined several collaborators for two sessions.
In the first, titled “Joint-Symposium Breakthrough T1D (formerly JDRF)-ISPAD: Type 1 Diabetes (T1D) Treatments: Hope and Promise Ahead,” two recipients of ISPAD/Breakthrough T1D fellowships, which allow care providers to travel to and receive training at world-class diabetes centers, shared their experiences and how the fellowship enabled them to improve the care they can provide to their communities.
After a presentation from Chantal Matthieu, a longtime Breakthrough T1D investigator, partner and reviewer, Dr. Dutta presented an overview of our work, our vision, and how the next generation of researchers in the room can apply for funding and join us in our work.
In the second session, the Joint ISPAD – Breakthrough T1D symposium, Dr. Dutta and others provided an update on our progress in treating this disease and what’s on the horizon. They touched on the many ways we can slow down disease progression, the exciting state of stem cell-derived cell therapies (they’re in human clinical trials and they’re producing insulin), and how artificial intelligence can play a role in reducing or eliminating T1D misdiagnosis in adults which can be as high as 40%.
Key takeaway:
It’s an exciting time in T1D research, and Breakthrough T1D’s strategy has mapped out what it takes to get to cures—including the importance of bringing in the next generation of researchers to contribute.
Revolutionizing Diabetes Care: Cutting-Edge Therapies
This session, which was a personal favorite of the author, gave updates on the biggest priorities we have at Breakthrough T1D: cures and how close we are to realizing them.
Spoiler alert: we’re not that far away.
It featured presentations from several Breakthrough T1D-funded researchers, including Colin Dayan, MD, Lori Laffel, MD, and Kimberly Simmons, MD.
First up: Dr. Simmons spoke about Tzield, the first disease-modifying therapy approved for T1D, and its use in the real world. A quick summary of the data:
- 322 people have received the drug to date
- The side effects reported in the clinical trial are consistent with what has been seen at the Barbara Davis center
- “Most of our patients have told us that they would do this treatment again.”
- Long term data for how people are tolerating the therapy and progression to T1D is not available yet.
As a reminder, Tzield was FDA-approved in November 2022 for individuals with stage 2 T1D to delay onset by an average of two years. Learn more in this comprehensive story on how it came to be and the role Breakthrough T1D played in getting it to market.
Dr. Michael Rickels then explored cell replacement therapies: where we are and where we’re going. His presentation covered the current landscape: We can use cadaveric islets to restore insulin production in people with T1D. However, the requirement for chronic immunosuppression and scarcity of donor islets mean this is not a viable option for the vast majority of people with T1D.
The next step is using an unlimited supply of stem cell-derived islets and discovering methods to keep them safe without the use of chronic immunosuppression, which is consistent with our strategy in this area.
Dr. Rickels also touched on the study that used autologous cells to restore insulin production in a person with T1D.
Lastly, Dr. Colin Dayan gave an update on combination therapies to preserve beta cell function in people with T1D.
Combination therapies utilize several different therapies that work by discrete mechanisms to target a singular problem. An example is tuberculosis or HIV, which both relied on complicated treatments composed of different pills that had to be taken at different times of day but are now treated with singular pills.
As we have shown, there are many drugs that can preserve insulin production. Now we’re learning which drugs can be taken together to preserve that insulin production longer. Dr. Dayan discussed the T1D Plus study (which builds on the Ver-A-T1D trial), which is funded by Breakthrough T1D, JDRF Australia, INNODIA, and the Helmsley Charitable Trust. This study will test several different drug combinations to see their effectiveness, including Tzield, verapamil, antithymocyte globulin (ATG), and golimumab.
Not only will this trial test multiple drugs—the innovative design of the study will speed up the length of the study, shaving years of the time it will take to see what combinations work best.
Key takeaway:
Breakthrough T1D is at the center of cell therapies and disease-modifying therapies. The clinical trials being run in humans today are very exciting and are a glimpse into how this disease could be treated in the not-too-distant future. It’s possible there will be approved combination therapies to slow progression and cell replacement therapies that restore insulin production entirely in the not-too-distant future.
Until next year!
These are just a few highlights from three days of sessions and presentations that cover our entire research portfolio. For example, Dr. Danne presented on the importance of early detection due to its numerous, clearly defined benefits and strategies for identifying these youths with stage 1 and stage 2 T1D. There were also sessions on the impact of AID systems, specific areas of complications, and much, much more.
We’re already looking forward to next year!
It’s early October, which means the Nobel Prizes are being awarded in several categories. These prestigious awards recognize outstanding contributions in Peace, Literature, Physics, Chemistry, Physiology or Medicine, and Economic Sciences. They go to the best and brightest people with the best and brightest ideas.
This year, the prizes recognize work that is, in several ways, connected to Breakthrough T1D and the work we are doing to cure type 1 diabetes (T1D) and improve the lives of those living with it.
microRNAs
The 2024 Nobel Prize in Physiology or Medicine was awarded to Victor Ambros and Gary Ruvkun for the discovery of microRNA and its role in post-transcriptional gene regulation.
But what is it?
The DNA in our body has between 20,000 and 25,000 genes. Our body constantly activates those genes, which allows it to function. For example, there is a gene that tells the beta cells to start creating insulin in response to elevated blood glucose levels.
This is called gene expression—it’s when the body produces something, usually a protein, to do something specific in the body. Gene expression happens when the DNA of a gene is copied to form messenger RNA, or mRNA, which is then turned into a protein that has a unique function. This is orchestrated in a highly tissue-specific manner, creating diverse cell types like muscle, nerve, beta cell, and more.
In 1993, we learned that molecules called microRNAs regulate gene expression. They can hamper or promote it. By measuring the presence of microRNAs and using them as a biomarker, we can learn a lot about what is going on inside the body, what genes are being expressed, and in which cell types.
How does this apply to type 1 diabetes?
Breakthrough T1D is actively funding research into the use of microRNAs to advance our mission. In fact, we are currently funding $2.6 million in grants related to microRNAs. Specifically, we’re exploring their use as biomarkers of disease progression and as a therapeutic target to interfere with the autoimmunity behind T1D.
Biomarkers
Biomarkers are, put very simply, things in the body that can be measured. Pulse, body temperature, and blood pressure are all biomarkers. In T1D, there are a handful used in common parlance: blood glucose level, HbA1c, time-in-range, autoantibody status, and more. We want to validate the use of microRNAs as a biomarker of disease progression.
We know through years of work that early detection has many benefits. This includes being educated on what T1D is, preparing for a potential diagnosis, the ability to benefit from a disease-modifying therapy to delay onset, and preventing potentially life-threatening complications at onset. microRNAs have the potential to increase our understanding of disease progression and identify how quickly a person is progressing.
Type 1 diabetes occurs in stages. Today, biomarkers of progression, like autoantibody status, don’t paint the whole picture. If a person tests positive for 2 autoantibodies, that means they are almost 100% likely to develop T1D at some point—but we don’t know how fast. We can measure blood glucose levels, but that is a single data point for dysglycemia. It doesn’t tell us how healthy the beta cells are.
microRNAs have the potential to paint a much more detailed picture. We are funding research to discover whether we can use microRNAs to learn exactly where a person is in their progression to stage 3 T1D and how quickly it’s happening.
In summary—we believe microRNAs can enhance the predictive value on top of the current biomarkers for T1D. They can be a very useful tool in measuring progression and helping people in stages 1 and 2 of T1D.
microRNAs as a therapeutic target
Type 1 diabetes is an autoimmune disease—a disease where the body’s immune system destroys its own cells. In T1D, the T-cells in the immune system destroy the insulin-producing cells in the pancreas.
Our research into stopping disease progression focuses mainly on two areas: modifying the immune system and modifying the beta cells. microRNAs can potentially help us fix the dysregulation in the immune system, slowing down or halting the autoimmune attack.
Breakthrough T1D-funded researchers discovered that blocking microRNA-146a in mice can prevent the T-cells from damaging the beta cells. Preventing damage to the beta cells prevents T1D from progressing. Our hypothesis: if we can block microRNA-146a, we can slow down or halt disease progression. This specific study is in a pre-clinical setting, and if it goes well, it could move into clinical trials in the near future.
David Baker – Nobel Prize in Chemistry
David Baker, a breakthrough T1D-funded researcher, was awarded half the 2024 Nobel Prize in Chemistry for computational protein design.
Baker’s prize acknowledges his work in discovering a way to create new proteins that have never existed before. These proteins can potentially be used to treat diseases, make new vaccines, and more. A few years ago, we saw a potential application to T1D.
There haven’t been any groundbreaking changes in insulin since the discovery of synthetic insulin in the late 1970’s. Breakthrough T1D wants to change that—and is funding researchers, like David Baker, to figure out what the next generation of insulins can look like.
Baker received two grants from us from 2016-2021 to use a computer model to create new, glucose-responsive insulin (GRI). GRI is insulin that can be administered, exist in the blood stream, and only be active when it is needed. Baker’s grant was one of many projects we are pursuing in GRI. This work continues to this day, and there are even GRIs in human clinical trials.
What’s next?
This year’s Nobel Prizes show that we are focusing on the same things the Nobel Committee is focused on: the best and brightest scientists and the best and brightest research. Hopefully, one day, we’ll see a T1D scientist win a Nobel Prize for curing this disease.
Want to learn more?
Visit our Funded Research page, where you can read about every single grant we fund—including David Baker’s work in GRI and the many grants currently being funded to study microRNAs.
After a type 1 diabetes (T1D) diagnosis, the first question that often comes to mind is, “Will there ever be a cure for type 1 diabetes?”
There is currently no type 1 diabetes cure. There is also currently no way to prevent its onset. But Breakthrough T1D has a strategy to change this and we’re already seeing exciting results. Here’s how we’re transforming the future for everyone with T1D:
Curing T1D: Cell Therapies
The Breakthrough T1D Cell Therapy Program invests in research and clinical trials to develop and deliver life-changing therapies that place healthy, insulin-producing cells back into the bodies of people with type 1 diabetes. The program has three goals that identify the gaps we’re filling to make a type 1 diabetes cure a reality:
- Develop a reliable beta cell source so that there are enough cells for every person with T1D to get this treatment.
- Find ways to support the beta cells so they stay healthy and functional in the body for an infinite amount of time.
- Shield the beta cells from immune attack to prevent the need for additional immunosuppressive drugs.
Learn more about Breakthrough T1D’s research advancements in cell therapies.
Halting, Preventing, and Reversing T1D: Disease-Modifying Therapies
Breakthrough T1D is also focused on developing drugs that change the course of T1D for everyone affected by it—and those yet to be. That means slowing or halting the progression of the disease, preventing it from ever occurring, and reversing it entirely.
In November 2022, the FDA approved Tzield, the first disease-modifying drug for individuals at risk of developing T1D (those who have tested positive for T1D antibodies). The therapy changes the disease’s course by delaying the onset of T1D for approximately two years. This is a tremendous leap forward for T1D and autoimmune research and a step closer towards type 1 diabetes cures.
Learn more about Breakthrough T1D’s progress in disease-modifying therapies.
Better Health Outcomes: Global Universal Screening
Screening is another key component of using research to find a cure for type 1 diabetes. Thanks to Breakthrough T1D-funded research, we have a better understanding of the human immune system. We can now identify a person’s risk for T1D many years before the onset of symptoms through a simple blood test that detects T1D autoantibodies, an established marker of risk of developing the disease. This makes it possible to prevent serious illness, like diabetic ketoacidosis (DKA), that often comes with a type 1 diabetes diagnosis.
By identifying more people in the early stages of T1D through screening, researchers can learn more about the progression of the disease and how to delay and prevent it from occurring. It’s another important step towards type 1 diabetes cures.
Learn more about the important role screening plays in achieving a world without T1D.
Improving Lives Today and Tomorrow for Everyone with T1D
While our focus is on finding cures for type 1 diabetes, we’re also in constant pursuit of new treatments to keep people with T1D healthy until that day comes.
Drugs and Devices
Technology has changed the way we live with T1D. Continuous glucose monitors (CGMs), insulin pumps, and artificial pancreas systems have made managing the disease easier. Next-generation insulins have the potential to work faster and automatically respond to changes in blood glucose. Breakthrough T1D continues to invest in innovative research and technology to improve outcomes and quality of life for people with T1D while we pursue cures for type 1 diabetes.
Learn more about Breakthrough T1D’s progress in developing drugs and devices for glucose control.
Advocacy
Outside of the research lab, we push for increased government funding for research. We also work with academia, clinicians, insurers, and regulators to get new therapies and devices to market quickly and safely, and ensure they’re covered by payers.
Learn more about Breakthrough T1D’s advocacy initiatives.
We’re closer than ever to freeing people with T1D from the burden of the disease. Breakthrough T1D exists to find type 1 diabetes cures, and we will not stop working until that goal is achieved.